Scientific knowledge is by nature dynamic and doubtful; it is never a certainty: "In a sense, all truth is only an error that corrects another error" (V. Frankl). It progresses through successive tests and constant corrections, like a cybernetic robot. The human activity of knowledge never leads to an image of phenomena that is certain and true, but only to a conjectural interpretation of phenomena characterised by their regularities [14]. Karl Popper described it well: "Science does not rest on a rocky foundation. The bold structure of its theories is built, as it were, on a swamp. It is like a building on stilts. The stilts are driven into the swamp, but only until they hit a natural or 'given' base, and when we stop trying to drive them further in, it is not because we have reached firm ground. We stop only because we are convinced that it is solid enough to support the building, at least temporarily" [10]. Every scientific theory can be challenged by a new observation or a new paradigm; it is never "ultimate", but always temporary, provisional and open to attack, "falsifiable" as it is called [11]. All scientific thought also depends on a set of concepts, tacitly accepted and shared by the intellectual community, which constitute the paradigm currently in force in society. All research and observations are conceived and interpreted in terms of this paradigm, which is the mental framework within which the thinking of the time develops. Because it is structured and coherent, this paradigm changes little, but it can collapse in the face of discoveries that contradict its foundations [7]. It then gives way to a new paradigm, during one of the scientific revolutions that mark history, such as those of Galileo, Copernicus, Pasteur or Einstein.
This raises a fundamental question: under what circumstances can conclusions be considered valid ? To be valid, they must fulfil a number of conditions [4]:
- Your database is a collection of objective data that can be analysed statistically;
- This data can be organised into a coherent theory;
- This theory predicts certain observations that can actually be made;
- These observations can be replicated by other teams.
In the field of anaesthesia, the first point is fulfilled by the numerous retrospective or prospective experimental and clinical studies whose statistical results, specific to each of them, are undeniable achievements. Their organisation into coherent theories is currently much more complex. A theoretical explanation is a proposal that reformulates observations into a system of concepts acceptable to a group of experts who share the same validation criteria [8]. Apart from the rigour of the observation and the logical consistency of the conclusions, these criteria are often poorly defined in medicine. Prediction of observations - the third point - is naturally limited in systems as complex as a human organism undergoing the stress of surgery. As for the last point, the medical literature of the last twenty years is full of cardiovascular studies whose results have never been reproduced.
This is not surprising, as the haemodynamic equilibrium is a multifactorial system in constant readjustment. Our measurements only capture the result of complex interactions and feedbacks between a large number of factors. In complex systems, causality is no longer linear, but multiple and interdependent: a change in one element of the system may or may not have consequences depending on the state of the other elements of the system with which it interacts. The fundamental logical error is to confuse essential participation with sole responsibility [8]. For a breakdown or accident to occur, several elements must be affected: each change reduces the safety margin of the whole, but is not in itself the triggering cause. In fact, it is not surprising that it is so difficult to identify independent predictive factors, for example when estimating operational risk, because the classical method of investigation only allows you to study a relationship once it has been isolated from the complex whole of the overall system. However, the choice of a single axis of analysis transforms the observed object into a dominant mode of causality, because the multiple regulations operating within the system are reduced to a minimum [1]. The observed relationship has predictive value only in the particular context of that analysis; it is highly unlikely to be reproducible in another context [12].
Causality can take two very different forms. Deterministic causality is characterised by a direct relationship between cause and effect; in this system the cause is the necessary and sufficient element for the effect to occur. Every time the cause is repeated, the effect is repeated. It is by isolating a simple phenomenon and observing its evolution that the scientific theories of classical physics and biology have been constructed. But the phenomenon is only simple to our minds, and the laws we deduce from our observations are merely the translation into language of an observation that appears to us as such because we have excluded all other elements from our experience. The question we ask determines the answer we get. We cannot know whether our deduction corresponds to a reality in the world, or whether it is simply a statistically coherent interpretation within a preconceived mental system. Probabilistic causality, on the other hand, does not maintain a direct and unambiguous relationship between a cause and an effect. The same cause may produce a different effect depending on the context. Several mechanisms are required to produce the effect, but they are themselves interdependent. The observed phenomenon is therefore multifactorial in origin and cannot be isolated from its context. There is even a fundamental uncertainty about the possibility of determining the sequences that lead to the observed effect. It is true that we can trace the sequence of events that led to a phenomenon in an attempt to explain it, but this is not the only possible chain of events. What is right in one case may be wrong in another. An isolated success is no guarantee that the theory is adequate. As a result, it is impossible to predict how the many elements in play will come together to anticipate what will happen. History is the best illustration of this: it can explain everything by going back in time, but it cannot predict anything by extrapolating into the future. It works in reverse: it defines causal chains because it reconstructs causes from effects. It is always right because it already knows the future of events when it looks for their origins. Like any case presentation in a morbidity-mortality debate, it is constantly threatened by the trap of 'post hoc ergo propter hoc' (after this, therefore because of this), which attributes a causal relationship to the simple temporal succession of two phenomena. The human mind, curious and anxious from the outset, needs to find coherence in the world around in order to cope with it; it easily confuses a possible explanation with a formal proof.
The measuring instrument itself determines the results. We do not observe nature itself, but nature subjected to our methods of investigation [5]. And it is the observer who sets the parameters. In anaesthesia, for example, the traditional "pressure-flow" reading system (Swan-Ganz catheter) observes haemodynamics from its own point of view, but does not allow us to see all the phenomena. Another system, such as the 'flow-volume' data provided by echocardiography, takes measurements from a different angle and can give different interpretations of the same situation. The sensitivity and specificity of each method varies according to the type of lesion and the class of patient: The ECG, which analyses the electrical changes associated with variations in coronary flow, has different sensitivities depending on the type of ischaemia. It is pointless to decide arbitrarily that one method of observation is the gold standard; the point is to use them together, so that they complement each other, and in this way build up bits and pieces of the most adequate model of reality.
This dependence on the system of observation has direct clinical consequences. Depending on whether CK-MB levels, WHO criteria (angina, ECG changes and CK-MB elevation), troponin I or troponin T are used, the incidence of postoperative myocardial infarction varies between 1.4%, 3%, 12% and 17%, respectively [6,13]. Minimal elevation of high-sensitivity troponins (TnT-hs 0.03-0.4 ng/ml) is present in 8-19% of patients at risk after surgery, although 58% of them do not meet the criteria for infarction and 84% are asymptomatic. They suffer from what is known as MINS (Myocardial Injury after Noncardiac Surgery) [2,9]. This phenomenon is associated with a threefold increase in cardiovascular mortality and an improvement in prognosis when conventional treatment of ischaemia is initiated [3]. In this case, the problem is to know whether a measurement system is overestimating the incidence of the condition. Increasing sensitivity sacrifices specificity: there is a risk of treating conditions that do not exist. What's more, we tend to confuse the marker of a phenomenon with the phenomenon itself. Troponin is not heart attack, CEA is not colon cancer, and the BIS™ is not the patient's sleep. The geographical map is not the territory! On the other hand, the problem is more fundamental: we fragment reality into a multiplicity of entities defined by our language, which we rely on to find our way around, whereas reality is a complex cross-fade to which we have access only through the representations we make of it (Figure 1.5).
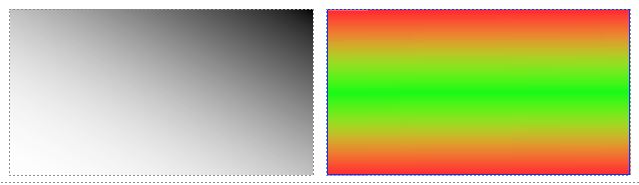
Figure 1.5: Examples of cross-fading. In the figure on the left, it is clear that the top right corner is black and the bottom left corner is white, but the boundary between the two colours is a progressive gradient in the density of black pixels which makes it impossible to draw a distinct boundary between black and white. The diagonal of the rectangle, which is the statistical median of the balanced grey, can be considered as an arbitrary boundary because the figure is of simple geometry. The figure on the right is already more complicated, since there are two horizontal transitions between red and green without it being possible to assign a geometric boundary to the two colours, although it is obvious that the edges are red and the centre green.
In reality, forms, processes and diseases are infinitely more complex than those shown in the diagram. But the problem is the same: defining a colour zone, like defining a heart attack, consists of drawing a boundary within which the entity in question exists and beyond which it does not. This boundary has no real existence; it marks a boundary between entities that we define in order to represent them with discrimination and manipulate them with precision. But what is wrong from an ontological point of view is still useful from a pragmatic point of view. Nevertheless, the desire to circumscribe and define things prevents any direct access to reality and means that we can only know our representation of the world, not the world itself. Do MINS correspond to a nosological reality? The answer to this question can only be a tautology, since the language that defines the phenomenon is the same as that which codifies our representation of myocardial ischaemia. We are prisoners of the convention that reality can be broken down into small autonomous entities that we define, name and combine to build a coherent pathophysiological edifice for our reason. These entities maintain a relationship to reality at a distance analogous to that which both separates and connects the word and the object it describes. But this is only one possible reading of reality. All we can say is that it works quite well in our conception of the world, which is only one out of many.
| Some epistemology |
| Science is a language that describes our representations of the world, based on the regularity of phenomena to which we ascribe the status of law. Scientific 'truths' are never acquired certainties, but are by their very nature open to challenge by new discoveries. The linear relationship between cause and effect is verifiable only in simple systems artificially isolated from their context. The complex systems analysed by medicine are based on multifactorial or probabilistic causality. Their study depends fundamentally on the measuring instrument used.
In order to manage it according to our paradigms, we fragment reality, which is by nature continuous, into isolated and defined entities that form the basis of physiopathology and nosology. These entities correspond to the way our reason works; they have the same distance from reality as that which separates the object from the word that describes it. |
© PG Chassot April 2007, last update September 2019
References
- AMZALLAG GN. La raison malmenée. Paris, CNRS Edition, 2002
- BOTTO F, ALONSO-COELLO P, CHAN MT, et al. Myocardial injury after noncardiac surgery: a large international prospective cohort study establishing diagnostic criteria, characteristics, predictors, and 30-day outcomes. Anesthesiology 2014; 120:564-78
- FOUCRIER A, RODSETH R, AISSAOUI M, et al. The long-term impact of early cardiovascular therapy intensification for postoperative troponin elevation after major vascular surgery. Anesth Analg 2014; 119:1053-63
- HAYWARD JH. Scientific method and validation. In: HAYWARD JW, VARELA FJ. Gentle Bridges. Shambala Ed., Boston, 1992
- HEISENBERG W. Physics and philosophy, the revolution in modern sciences. Harper, New-York, 1958
- KEMP M, DONOVAN J, HIGHAM H, HOOPER J. Biochemical markers of myocardial injury. Br J Anaesth 2004; 93:63-73
- KUHN TS. The structure of scientific revolutions. Chicago: University of Chicago Press, 1962
- MATURANA HR, VARELA FJ. The Tree of knowledge. Shambala, Boston, 1992
- OBERWEIS BS, SMILOWITZ NR, NUKALA S, et al. Relation of perioperative elevation of troponin to long-term mortality after orthopedic surgery. Am J Cardiol 2015; 115:1643-8
- POPPER K. La logique de la découverte scientifique. Payot, Paris, 1973
- POPPER K. L'Univers irrésolu, plaidoyer pour l'indéterminisme. Hermann, Paris, 1984
- PRASAD V, VANDROSS A, TOOMEY C, et al. A decade of reversal: an analysis of 146 contradicted medical practices. Mayo Clin Proc 2013; 88:790-8
- PRIEBE HJ. Triggers of perioperative myocardial ischemia and infarction. Brit J Anaesthesiol 2004; 93:9-20
- WATZLAWICK P. L'invention de la réalité. Contribution au constructivisme. Seuil, Paris 1988