The heart must be stopped to allow for coronary anastomoses or opening of the heart chambers. O2 consumption should near zero when the aorta is clamped and coronary perfusion stops.This is achieved by cooling the heart externally with Hartmann's solution to 4-6°C (known as "Shumway") and perfusing internally with a cardioplegic solution (see Cardioplegic arrest and Cardioplegic techniques). This solution is essentially a cold water or blood compound containing potassium (20-30 mmoles/L). 10 mL/kg or 450 mL/m2 will stop the heart. It is delivered by a dedicated pump on the bypass machine or formerly by a pressure cuff (Figure 7.13).
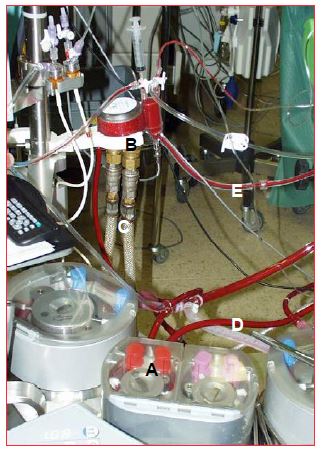
Figure 7.13: Cardioplegia circuit. A: Cardioplegia pump. B: Cardioplegia heat exchanger. C: cooling circuit. D: arterial blood supply from the general circuit. E: return of blood to the cardioplegia cannula.
There are several techniques for circulating cardioplegia through the coronary tree.
- Cardioplegia cannula in the aortic root, upstream of the aortic clamp; if the aortic valve is competent, the cardioplegia fills the aortic root under pressure (70-150 mmHg) and perfuses the coronary trunks at a rate of about 200-400 mL/min In the case of even minimal aortic insufficiency (AI), cardioplegia leaks under pressure into the LV and dilates it as soon as it slows and stops beating (see Figure 7.32 and Figure 7.40). This can be prevented by continuous TEE monitoring of the LV. It can also be prevented by placement of a drainage cannula in the LA.
- Spencer cannulae; when operating on the aortic valve or the root of the aorta, the coronary trunks can be perfused directly with cannulae inserted into the coronary ostia. This system presents a risk of embolisation of atheromatous material and a risk of coronary dissection, but eliminates the risk of ventricular leakage in case of AI. Perfusion pressure: 70-150 mmHg.
- Retrograde cardioplegia; using a cannula including a soft sealing balloon, the coronary sinus can be cannulated through the RA. Indicated in case of severe proximal coronary stenosis, non-collateralisation or aortic insufficiency. As blood from the RV drains directly into the ventricular cavity and the RA, retrograde cardioplegia does not protect the free wall or basal wall of the RV and is therefore most often combined with anterograde cardioplegia. Perfusion pressure is carefully monitored, as it should not exceed 30-40 mmHg at a flow rate of 100-300 mL/min since this is a venous and not an arterial network [1].
- Cardioplegia through bypass grafts: once the distal anastomosis has been performed, the venous bypass grafts can be perfused with a cardioplegic solution to protect the revascularised myocardium.
| Cardioplegia |
| Cardioplegia is a cold potassium enriched solution that stops the heart in diastole. It is injected through the root of the aorta (in the absence of aortic insufficiency), by cannulation of the coronary trunks, retrogradelly in the coronary sinus, or through the venous bypasses. It is perfused by a pump and a heat exchanger separate from the main bypass circuit. |
© CHASSOT PG, GRONCHI F, April 2008, last update December 2019
References
- HONKONEN EL, KAUKINEN L, PEHKONEU EJ, et al. Myocardial cooling and right ventricular function in patients with right coronary artery disease: antegrade vs retrograde cardioplegia. Acta Anaesthesiol Scand 1997; 41:287-95