Due to the extreme diversity of cardiac malformations, classification is necessary. It is useful to refer to the basic segmental analysis concept adopted by anatomical pathologists. This divides the heart into three segments [10,12]:
- The atrial segment, which includes the atria and the great veins;
- The ventricular segment, which includes the ventricles and atrioventricular valves;
- The arterial segment, which includes the aorta and the pulmonary artery with their respective valves.
These three segments are joined by two junctions (Figure 15.1):
- The atrioventricular junction;
- The ventriculoarterial junction.
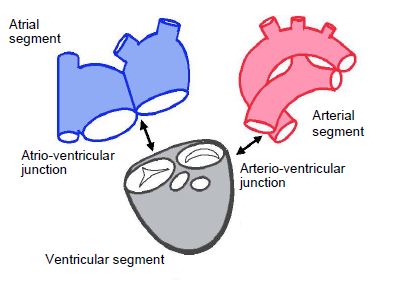
Figure 15.1: Segmental analysis of the heart. The heart is divided into three segments (atrial, ventricular and arterial) connected to each other by 2 junctions (atrioventricular and ventriculoarterial junctions). The venous return is part of the atrial segment. The atrioventricular valves are part of the ventricular segment and the ventriculoarterial valves are part of the arterial segment [4].
Each segment is defined by its intrinsic morphology since it is not possible to reliably identify the cardiac chambers based on their position and size, because: each of them may be repositioned, atrophic, hypertrophied or even absent. Five criteria are used to determine the heart's anatomical structures [5].
- Situs – this may be solitus (normal) or inversus (heterotaxy) – since the heart's situs is consistent with abdominal situs (except in very rare cases that never reach adulthood), it is essentially defined by the position of the right atrium (RA), which receives the inferior vena cava (IVC) or, in the absence of an IVC, the hepatic veins from the liver. The incidence of heterotaxy is 0.8 per 10,000 births [6].
- Concordance or discordance of two successive segments – instead of succeeding each other in a normal position (concordance), two segments may be in an inappropriate relative position (discordance), with the left-right axis of one at 180° to that of the other.
- Segmental connections – the junctions between segments are the atrioventricular canal between the atria and ventricles and the infundibulum between the ventricles and arteries.
- The specific markers of each cardiac chamber – for example, the LV is defined by the presence of two papillary muscles, a bicuspid mitral valve, fine trabeculation, and a partially fibrous outflow tract.
- Associated anomalies – these include dysmorphic structures, obstructive lesions, and defects in a septum (shunting).
The anatomical descriptions of structures and pathologies provided in this chapter are based mainly on echocardiographic imaging [2,3,7,9,11,13]. They are illustrated by diagrams and images obtained by transesophageal echocardiography (TEE).
Atrial segment
The cardiac situs is determined by the position of the atria. In the vast majority of cases, it is the same as the abdominal situs, with transdiaphragmatic discordances occurring only in severe and very rare pathologies that are not encountered in adults. The RA can be identified by the junction with the inferior vena cava (IVC) – if the IVC is absent, the hepatic veins flow into the RA. The RA and the liver, which are both easily identifiable, are therefore on the same side. The pulmonary veins may anastomose elsewhere than into the left atrium (LA) in cases of anomalous pulmonary venous return.
The atria may also be distinguished by their specific anatomy. The RA has a short, obtuse and pyramidal atrial appendage. It is the site of the fossa ovalis of the atrial septum and receives the insertion of the Eustachian valve. Its wall is partially trabeculated. The boundary between the smooth part and the trabeculated part is marked by a crest (crista terminalis), which runs from one vena cava to the other (Figure 27.129). The LA, whose wall is completely smooth, has a long, pectinate, finger-shaped atrial appendage. Sometimes both atria exhibit the same anatomical characteristics, which is described as isomerism or mirror-image atria. Right isomerism (two RAs) is normally associated with the absence of the spleen (asplenia), while left isomerism (two LAs) is characterised by multiple spleens (polysplenia) [6].
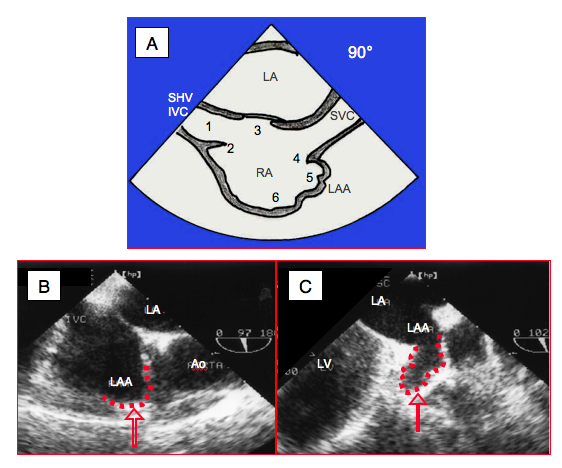
Figure 27.129: Anatomical criteria for the definition of right atrium (RA). A: Transesophageal bicaval view (90-100°). 1: IVC: inferior vena cava, SHV: supra-hepatic vein. 2: Eustachian valve. 3: fossa ovalis. 4: crista terminalis. 5: left atrial appendage (LAA). 6: trabeculated part of RA. B: right atrial appendage (bicaval view). C: left atrial appendage (2-chamber view).
Atrioventricular junction
The junction between the atrial septum, interventricular septum, septal leaflet of the tricuspid valve and anterior leaflet of the mitral valve forms the internal crux of the heart. These four structures may exhibit a coalescence defect, leaving an orifice in the centre of the heart – this is an atrioventricular canal (AV canal) or endocardial cushion defect. Normally, the septal insertion of the tricuspid valve is 5-10 mm distal to that of the mitral valve (0.7 cm/m2). Both valves are on the same plane in the event of atrioventricular canal defects (Figure 15.2) [8].
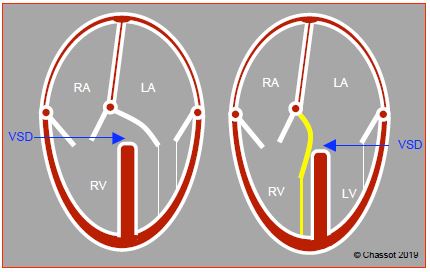
Figure 15.2: Atrioventricular junction. In normal circumstances, the septal insertion of the tricuspid valve is in a more apical position than that of the mitral valve. The difference is approximately 1 cm in adults (0.7 cm/m2). Both valves are on the same plane in cases of common atrioventricular canal defects (AV canal defects).
The atrioventricular junction is concordant if the atria and ventricles follow on from each other in the correct order. It is discordant if each atrium is connected to the contralateral ventricle. In the event of discordance, the tricuspid valve remains attached to the right ventricle (RV) and the mitral valve remains attached to the left ventricle (LV). If both atria are connected to a single ventricle, this is described as a double-inlet ventricle. If an atrioventricular valve opens into both ventricles due to a ventricular septal defect (VSD), this is described as “overriding”. This malformation may be supplemented by “straddling” if the valve’s chordae tendineae are inserted into a wall of the contralateral ventricle through the VSD (Figure 15.3).
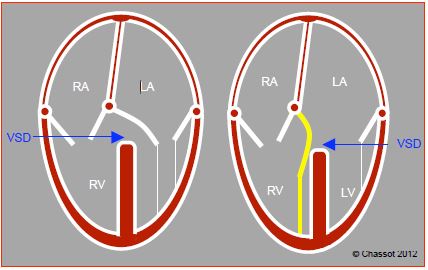
Figure 15.3: Atrioventricular junction. A: Overriding – the mitral valve overrides the septum, with its orifice anastomosing to both ventricles, although the subvalvular apparatus is on the same side. It is connected to the ventricle that receives > 50% of its surface area. B: Straddling – the subvalvular apparatus of the overriding valve, in this case the mitral valve, is inserted into both sides of the septum, with part of the chordae crossing the VSD.
Ventricular segment
A ventricle is composed of three parts: an inlet, a trabeculated body, and an outflow tract. A chamber that receives more than 50% of the opening of the corresponding atrioventricular valve is considered as a ventricle. Below this value, it is defined as a rudimentary chamber. Position, shape and size are unreliable indicators of which ventricle is right or left as these data may be profoundly disrupted. Other criteria are used to distinguish them (Figure 15.4) [3].
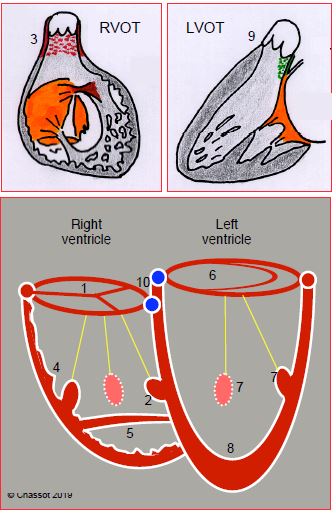
Figure 15.4: Differentiation of the RV and LV. The RV is connected to a tricuspid valve (1) and contains 3 (or more) papillary muscles, one of which is located on the septum (2); its outflow tract is entirely muscular (3); it exhibits significant trabeculation (4); and generally a clearly defined muscular moderator band (5). The LV is connected to a bicuspid valve (6) and only contains 2 papillary muscles (anterolateral and posteromedial, sometimes single) (7), neither of which is inserted on the septum; it is slightly trabeculated (8) and its outflow tract includes a fibrous continuity between the aortic valve and anterior leaflet of the mitral valve (9). The height difference between the septal insertions of the tricuspid and mitral valves (10) helps differentiate the RV (low insertion) from the LV (high insertion) (0-20° 4-chamber view). This indicator is lost if AV canal defects are present as both valves are inserted at the same level in patients with this pathology [1].
A right ventricle is distinguished by:
Atrial segment
The cardiac situs is determined by the position of the atria. In the vast majority of cases, it is the same as the abdominal situs, with transdiaphragmatic discordances occurring only in severe and very rare pathologies that are not encountered in adults. The RA can be identified by the junction with the inferior vena cava (IVC) – if the IVC is absent, the hepatic veins flow into the RA. The RA and the liver, which are both easily identifiable, are therefore on the same side. The pulmonary veins may anastomose elsewhere than into the left atrium (LA) in cases of anomalous pulmonary venous return.
The atria may also be distinguished by their specific anatomy. The RA has a short, obtuse and pyramidal atrial appendage. It is the site of the fossa ovalis of the atrial septum and receives the insertion of the Eustachian valve. Its wall is partially trabeculated. The boundary between the smooth part and the trabeculated part is marked by a crest (crista terminalis), which runs from one vena cava to the other (Figure 27.129). The LA, whose wall is completely smooth, has a long, pectinate, finger-shaped atrial appendage. Sometimes both atria exhibit the same anatomical characteristics, which is described as isomerism or mirror-image atria. Right isomerism (two RAs) is normally associated with the absence of the spleen (asplenia), while left isomerism (two LAs) is characterised by multiple spleens (polysplenia) [6].
Figure 27.129: Anatomical criteria for the definition of right atrium (RA). A: Transesophageal bicaval view (90-100°). 1: IVC: inferior vena cava, SHV: supra-hepatic vein. 2: Eustachian valve. 3: fossa ovalis. 4: crista terminalis. 5: left atrial appendage (LAA). 6: trabeculated part of RA. B: right atrial appendage (bicaval view). C: left atrial appendage (2-chamber view).
Atrioventricular junction
The junction between the atrial septum, interventricular septum, septal leaflet of the tricuspid valve and anterior leaflet of the mitral valve forms the internal crux of the heart. These four structures may exhibit a coalescence defect, leaving an orifice in the centre of the heart – this is an atrioventricular canal (AV canal) or endocardial cushion defect. Normally, the septal insertion of the tricuspid valve is 5-10 mm distal to that of the mitral valve (0.7 cm/m2). Both valves are on the same plane in the event of atrioventricular canal defects (Figure 15.2) [8].
Figure 15.2: Atrioventricular junction. In normal circumstances, the septal insertion of the tricuspid valve is in a more apical position than that of the mitral valve. The difference is approximately 1 cm in adults (0.7 cm/m2). Both valves are on the same plane in cases of common atrioventricular canal defects (AV canal defects).
The atrioventricular junction is concordant if the atria and ventricles follow on from each other in the correct order. It is discordant if each atrium is connected to the contralateral ventricle. In the event of discordance, the tricuspid valve remains attached to the right ventricle (RV) and the mitral valve remains attached to the left ventricle (LV). If both atria are connected to a single ventricle, this is described as a double-inlet ventricle. If an atrioventricular valve opens into both ventricles due to a ventricular septal defect (VSD), this is described as “overriding”. This malformation may be supplemented by “straddling” if the valve’s chordae tendineae are inserted into a wall of the contralateral ventricle through the VSD (Figure 15.3).
Figure 15.3: Atrioventricular junction. A: Overriding – the mitral valve overrides the septum, with its orifice anastomosing to both ventricles, although the subvalvular apparatus is on the same side. It is connected to the ventricle that receives > 50% of its surface area. B: Straddling – the subvalvular apparatus of the overriding valve, in this case the mitral valve, is inserted into both sides of the septum, with part of the chordae crossing the VSD.
Ventricular segment
A ventricle is composed of three parts: an inlet, a trabeculated body, and an outflow tract. A chamber that receives more than 50% of the opening of the corresponding atrioventricular valve is considered as a ventricle. Below this value, it is defined as a rudimentary chamber. Position, shape and size are unreliable indicators of which ventricle is right or left as these data may be profoundly disrupted. Other criteria are used to distinguish them (Figure 15.4) [3].
Figure 15.4: Differentiation of the RV and LV. The RV is connected to a tricuspid valve (1) and contains 3 (or more) papillary muscles, one of which is located on the septum (2); its outflow tract is entirely muscular (3); it exhibits significant trabeculation (4); and generally a clearly defined muscular moderator band (5). The LV is connected to a bicuspid valve (6) and only contains 2 papillary muscles (anterolateral and posteromedial, sometimes single) (7), neither of which is inserted on the septum; it is slightly trabeculated (8) and its outflow tract includes a fibrous continuity between the aortic valve and anterior leaflet of the mitral valve (9). The height difference between the septal insertions of the tricuspid and mitral valves (10) helps differentiate the RV (low insertion) from the LV (high insertion) (0-20° 4-chamber view). This indicator is lost if AV canal defects are present as both valves are inserted at the same level in patients with this pathology [1].
A right ventricle is distinguished by:
- The presence of a tricuspid valve inserted lower than the mitral valve at septal level (except if AV canal defects are present);
- Three (or more) papillary muscle(s), one of which has an insertion on the interventricular septum;
- Thick trabeculation and the presence of a moderator band (a muscular trabecula that crosses the chamber);
- A conical and entirely muscular outflow tract (infundibulum) – there is no continuity between the tricuspid and pulmonary valves.
A left ventricle can be identified by:
- The presence of a bicuspid (mitral) valve inserted above the tricuspid valve (except if AV canal defects are present);
- Two papillary muscles, sometimes fused into one, neither of which has an insertion on the interventricular septum;
- Finer trabeculation;
- A partially fibrous outflow tract with a fibrous continuity between the mitral valve and aortic valve.
Ventriculoarterial junction
The junction is concordant or discordant depending on whether or not the ventricle is connected to the appropriate vessel. Transposition of the great arteries (TGA) is the most common case of ventriculoarterial discordance: the RV is connected to the aorta and the LV to the PA (D-TGA). A double-outlet ventricle is characterised by a layout in which over 50% of a ventriculoarterial valve is connected to the same ventricle as the other vessel, whether this ventricle be right, left or single. While the valves may exhibit overriding, notably in the event of a membranous VSD as in tetralogy of Fallot, straddling is impossible as they have no chordae (Figure 15.5).
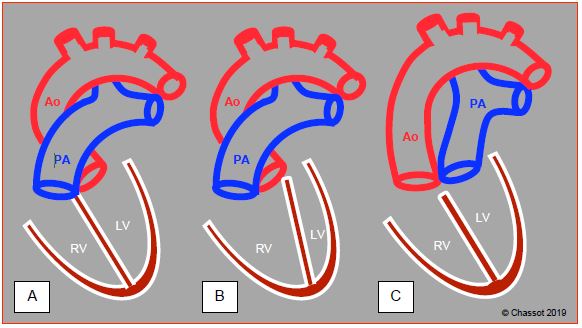
Figure 15.5: Pathologies of the ventriculoarterial junction. A: normal situation – the aorta (Ao) and pulmonary artery (PA) cross at 45°, whereby the PA is anterior. The PA can be identified by its division into two branches 4-5 cm after its origin. The ascending aorta is a long tube that has no branches before the vessels of the aortic arch. Since numerous coronary artery anomalies are possible, the positioning of the coronary arteries cannot be used as a criterion for identifying the aorta. B: double-outlet right ventricle (DORV) – due to the septum shifting, with or without VSD, both vessels originate from the RV. C: transposition of the great arteries (TGA) – the aorta emerges from the RV and the PA from the LV. On an echocardiogram, the two vessels are parallel in the long-axis view at 120° and the two valves are on the same plane in short-axis view (0-40°). Generally, the great arteries are parallel in the sagittal plane in cases of D-TGA (anterior aorta and posterior PA) and side-by-side in the frontal plane in cases of L-TGA.
Arterial segment
Two vessels emerge from the heart – the aorta, which is posterior, and the pulmonary artery (PA), which is anterior. In normal circumstances, they cross each other at their origin. While the aorta's first branches only emerge distally in the aortic arch, the PA splits into two branches after 4-5 cm. The coronary arteries are not a distinguishing feature as they may emerge from the aorta or the PA. If their embryonic septation has not occurred, the two vessels fuse to form a single vessel (truncus arteriosus) [6].
Shunts and obstructions
Shunting involves communication between the systemic and pulmonary circulation and may occur in different locations (see Shunts).
- Venous return: pulmonary vein drained into the RA;
- Atria: ASD;
- Crux of the heart: AV canal defect;
- Ventricles: VSD;
- Arteries: patent ductus arteriosus, aorta-PA collaterals.
Obstructions mainly occur in the two ventricles’ ejection pathways and in the aorta. They may be dynamic (concentric muscular hypertrophy of the outflow tract) or static (subvalvular membrane, valvular stenosis, arterial stenosis).
- Right pathway: dynamic stenosis of the RVOT, atresia or stenosis of the pulmonary valve, hypoplasia of the PA (typical of tetralogy of Fallot);
- Left pathway: membrane in the LVOT, aortic stenosis (bicuspid aortic valve);
- Aorta: coarctation
Obstructive lesions cause excessive afterload in the affected ventricle, which undergoes concentric hypertrophy. If a shunt is present, these modify the pressure ratio between the right and left circulations.
© BETTEX D, CHASSOT PG, January 2008, last update May 2018
References
| Nomenclature |
| In segmental analysis, the heart is divided into 3 segments (atrial, ventricular and arterial) and 2 junctions (atrioventricular and ventriculoarterial). The anatomical examination of congenital heart diseases is a 5-step process: - Defining the situs based on the RA - Defining the various chambers by their structures (number, position, development) - Examining the AV and ventriculoarterial junctions (concordance or discordance) - Checking for shunts - Checking for obstructive lesions |
© BETTEX D, CHASSOT PG, January 2008, last update May 2018
References
- ANDERSON R, HO SH: Echocardiographic diagnosis and description of congenital heart disease: Anatomic principles and philosophy. In ST JOHN SUTTON MG (ed): Textbook of echocardiography and Doppler in adults and children. Cambridge (MA): Blackwell Science, 1996, 711-743
- BETTEX D, CHASSOT PG. Transesophageal echocardiography in congenital heart disease. In: BISSONNETTE B, edit. Pediatric anesthesia. Basic principles, State of the art, Future. Shelton (CO): People’s Medical Publishing House (USA), 2011, 1186-1212
- BHATT AB, FOSTER E, KUEHL K, et al. Congenital heart disease in older adults. A Scientific Statement from the American Heart Association. Circulation 2015; 131:1884-931
- CHASSOT PG, BETTEX D. Perioperative transoesophageal echocardiography in adult congenital heart disease. In: POELAERT J, SKARVAN K. Transoesophageal echocardiography in anaesthesia. London, BMJ Book, 2004
- DUPUIS C, KACHANER J, PAYOT M. Cardiologie pédiatrique (Paediatric cardiology) Paris: Flammarion, 1991, 137-42
- KLOESEL B, DINARDO JA, BODY SC. Cardiac embryology and molecular mechanisms of congenital heart disease – A primer for anesthesiologists. Anesth Analg 2016; 123:551-69
- MILLER-HANCE WC, SILVERMAN NH. Transesophageal echocardiography (TEE) in congenital heart disease with focus on the adult. Cardiol Clinics 2000; 18:861-92
- PICCOLI GP. Morphology and classification of complete atrioventricular defects. Brit Heart J 1979; 42:633-9
- RUSSEL IA, ROUINE-RAPP K, STRATMANN G, MILLER-HANCE WC. Congenital heart disease in the adult: A review with Internet-accessible transesophageal echocardiographic images. Anesth Analg 2006; 102:694-723
- SHINEBOURNE EA, MACARTNEY FJ, ANDERSON RH. Sequential chamber localization. Logical approach to diagnosis in congenital heart disease. Brit Heart J 1976; 38:327-40
- STÜMPER O, SUTHERLAND GR. Transesophageal echocardiography in congenital heart disease. London: Edward Arnold, 1994, 37-38
- VAN PRAAGH R. Terminology of congenital heart disease. Glossary and commentary. Circulation 1977; 56:139-43
- WEYMAN AE. Complex congenital heart disease. I: diagnostic approach. In: WEYMAN AE. Principle and practice of echocardiography. Philadelphia: Lea & Febiger, 1994, 979-1001