In adults, diseases of the right ventricle outflow tract and pulmonary valve are extremely rare and are congenital in 95% of cases. The majority are lesions secondary to correction of tetralogy of Fallot, truncus arteriosus or congenital pulmonary stenosis. Rare acquired lesions include carcinoid syndrome, endocarditis, ARF and previous chest trauma [2]. In most cases, insufficiency dominates the pathology.
The pulmonary valve consists of three cusps which are mirror images of those of the aortic valve immediately behind it: the right cusp opposite the right coronary cusp, the left cusp opposite the left coronary cusp and the anterior cusp. These valves are located at the junction between the RV outflow tract (RVOT), which is an entirely muscular tube, and the root of the pulmonary artery (PA). The pulmonary valve has no fibrous ring and no direct anatomical relationship with the fibrous trine and rings of the other valves. Its mean diameter (measured in protosystole) is 2.4 cm in women and 2.6 cm in men [1]. It may be bicuspid.
The pulmonary valve is thin, not very echogenic and the most anterior of the valves, making it difficult to visualise on TEE. Its plane is practically perpendicular to that of the aortic valve: if one of the two valves is seen in the long axis, the other is seen in the short axis. The pulmonary valve is clearly visible in some views (Figure 11.161).
- 60° view of the inflow and outflow tract of the RV with slight rotation of the probe to centre on the root of the PA.
- 90° view of the middle oesophagus with clockwise rotation of the probe from a 2-cavity view of the LV.
- Short-axis view obtained from a long-axis view of the ascending aorta (120-160°) and slight green rotation to the right, or by 3D x-ray imaging; this view may be difficult to obtain.
- Short-axis view of the aortic arch at 90°, providing a long-axis view of the PA with the pulmonary valve at the bottom of the screen.
- Transgastric view of the RV at 40°; the pulmonary valve is an extension of the outflow tract of the RV.
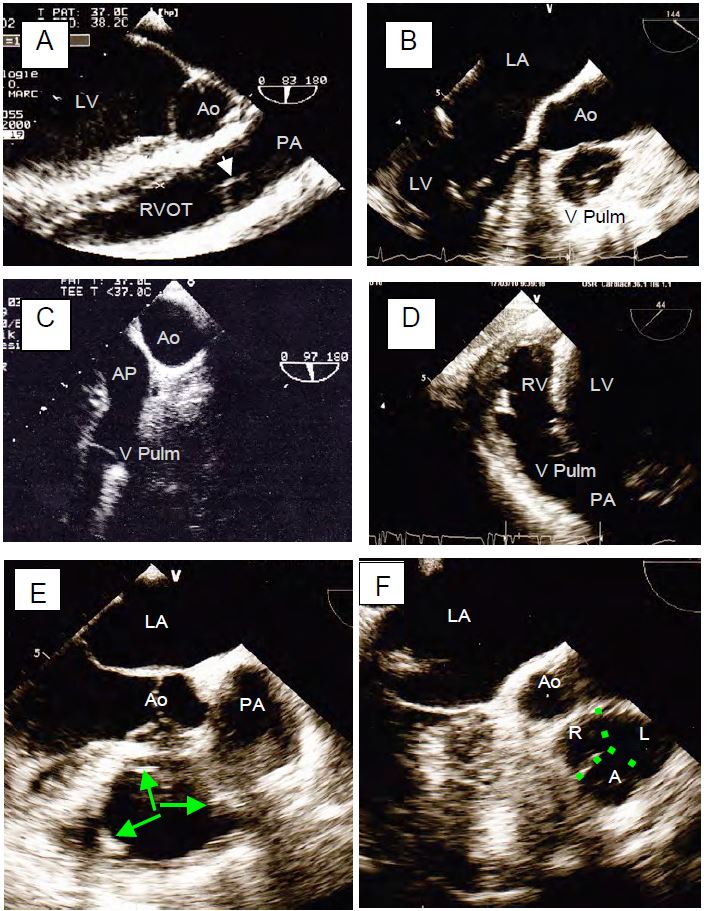
Figure 11.161: View of the pulmonary valve. It is not very echogenic because it is thin and very anterior and is partially obscured by the aortic valve. A: 90° mid-esophageal view by clockwise rotation of the probe from a 2-cavity view of the LV; the arrow indicates the level of coaptation of the cusps. B: Short-axis view obtained from a long-axis view of the ascending aorta (120-160°); the cusps are difficult to see. C: Short-axis view of the aortic arch at 90°, providing a long-axis view of the PA. D: Transgastric view of the RV at 40°; the pulmonary valve is an extension of the RV outflow tract. E: The short axis view of the pulmonary valve is difficult to obtain. In this view the 3 commissural points (green arrows) are at 3 o'clock, 7 o'clock and 11 o'clock. F: Identical view showing the 3 leaflets (right R, left L and anterior A).
| Pulmonary valve |
| The pulmonary valve lies anterior to the aortic valve and has 3 leaflets which are mirror images of the aortic cusps. It is poorly echogenic and very anterior, making it difficult to visualise on TEE. |
© CHASSOT PG, BETTEX D, August 2011, last update November 2019
References
- CAPPS SB, ELKINS RC, FRONK DM. Body surface area as a predictor of aortic and pulmonary valve diameters. J Thorac Cardiovasc Surg 2000; 119:975-82
- SCHILLCUTT SK, TAVAZZI G, SHAPIRO BP, DIAZ-GOMEZ J. Pulmonic regurgitation in the adult cardiac surgery patient. J Cardiothorac Vacs Anesth 2017; 31:213-28