Valvular heart disease progresses in two different directions: stenosis or insufficiency. Generally speaking, stenosis is more punishing than insufficiency because it imposes a haemodynamic restriction that does not allow cardiac output to adapt. The stroke volume becomes fixed and low and depends on the rate: bradycardia linearly reduces cardiac output and tachycardia prevents adequate filling in mitral stenosis or satisfactory ejection in aortic stenosis. On the other hand, insufficiency is less restrictive because the ventricles are good volume pumps and can cope with a certain degree of valvular regurgitation: they increase their stroke volume to compensate for the component that moves back and forth between systole and diastole. The maximum regurgitant fraction that the LV can chronically support without decompensation ranges from 30% in aortic insufficiency (AI) to 40% in mitral insufficiency (MI) [2]. Mild valvular insufficiency is common and of no clinical consequence; mild tricuspid, mitral and aortic regurgitation occur in 65%, 48% and 11% of the normal adult population respectively [1].
With age, the valves wear out, become fibrous, lose their flexibility and start to leak, like old engines leaking oil. In the case of the tricuspid valve or the pulmonary valve, this is not a major problem. In the case of the mitral valve, mild to moderate insufficiency is generally well tolerated and does not increase the risk of surgery, but it chronically increases the pressure in the RA and limits exercise tolerance. The prognosis depends largely on the mechanism involved. MI due to structural lesions in old age is generally stable, but functional MI is likely to vary considerably depending on left ventricular performance or the evolution of myocardial ischaemia. Other than mild aortic insufficiency, aortic insufficiency is more dangerous than MI because the volume overload occurs in a higher pressure regime: the diastolic pressure of the aorta is higher than that of the LA. The prognosis depends on the ventricular dimensions, since the ventricles compensate for the valvular insufficiency by dilatative hypertrophy and an increase in their telediastolic and systolic volumes.
In the case of polyvalvulopathy, the haemodynamic behaviour of the patient is determined by the dominant pathology. Put simply, we can say that
- Stenosis is more prevalent than insufficiency of the same severity;
- The pathology of the upstream valve determines the function of the downstream valve;
- If severe, mitral stenosis is the most restrictive pathology;
- The degree and type of ventricular remodelling on echocardiography can be used to assess the dominant pathology (Figure 11.14).
Anaesthetic management is based on the determination of the dominant pathology, as this will determine the patient's cardiovascular reactivity. Intraoperative echocardiography is invaluable in demonstrating how the heart compensates for valvular dysfunction.
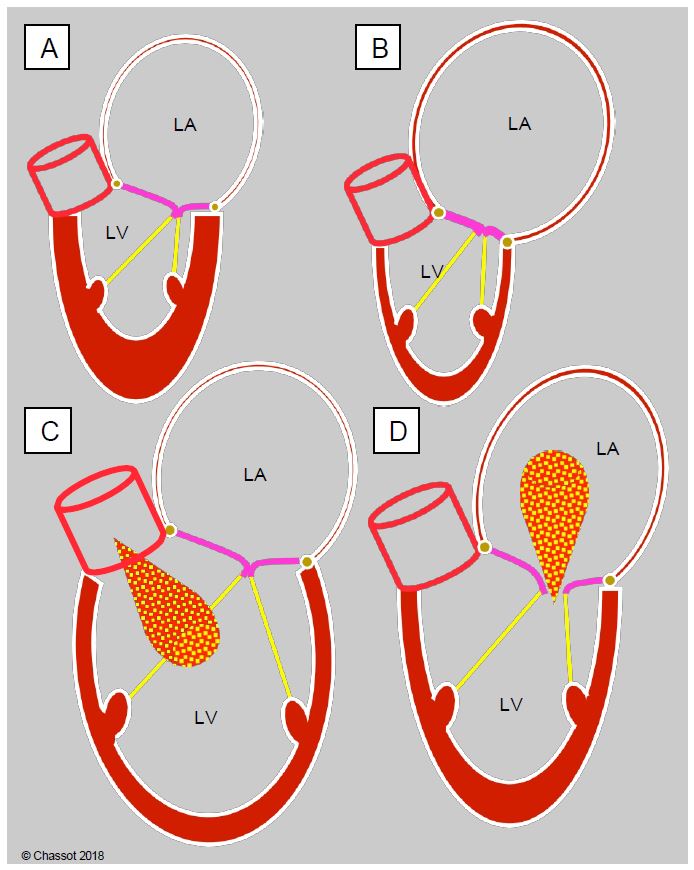
Figure 11.14: In the case of valvular disease, the silhouette of the cardiac chambers shows the remodelling of the left cavities as a function of haemodynamic constraints and makes it possible to determine the dominant pathology. A: aortic stenosis; concentric LVH and dilatation of the RA. B: mitral stenosis; small LV and gigantic RA. C: aortic insufficiency; massive dilatation of the LV, moderate dilatation of the RA. D: mitral insufficiency; dilatation of the LV and the RA
| Stenosis and regurgitation |
|
Stenosis is much more restrictive than regurgitation. Mitral regurgitation is better tolerated than aortic regurgitation.
With age, the valves often show mild insufficiency or sclerosis that limits their opening.
Haemodynamic behaviour depends on the dominant pathology:
- Stenosis is more severe than insufficiency.
- Upstream pathology controls downstream flow
- Mitral stenosis is the most frequent pathology.
The silhouette of the heart on echocardiography indicates the dominant pathology:
- Aortic stenosis: small LV (concentric LVH), dilatation of the RA
- Mitral stenosis: small LV and large RA
- Aortic regurgitation: massive dilatation of the LV, moderate dilatation of the RA
- Mitral regurgitation: dilatation of the LV (eccentric LVH), dilatation of the RA
|
© CHASSOT PG, BETTEX D, August 2011, last update November 2019
References
- KLEIN AL, BURSTOW DJ, TAJIK AJ, et al. Age-related prevalence of valvular regurgitation in normal subjects. A comprehensive color flow examination of 118 volunteers. J Am Soc Echocardiogr 1990; 3:54-63
- LANCELLOTTI P, TRIBOUILLOY C, HAGENDORFF A, et al. Recommendations for the echocardiographic assessment of native valvular regurugitation: an executive summary from the EACI. Eur Heart J Cardiovasc Imaging 2013; 14:611-44