Congenital stenosis of the left ejection pathway may be located at various sites:
- Subaortic in the LV outflow tract;
- Valvular, in the strict sense;
- Supravalvular at the root of the ascending aorta.
In addition to these lesions, others occur along the entire length of the thoracic aorta:
- Hypoplastic aortic arch, interrupted aortic arch (see Ventricular Hypoplasia);
- Shone’s syndrome;
- Coarctation of the aorta (see Coarctation of the Aorta).
Obstructed outflow tract
There are two types of fixed subaortic stenosis. The first involves a roughly circular membrane surrounding the outflow tract from the interventricular septum to the anterior leaflet of the mitral valve, and causes the equivalent of aortic stenosis (Video and Figure 14.62).
Video: Long-axis view of a membranous sub-aortic stenosis, visible as a fibrous crest on the septal wall of the left ventricular outflow tract; the aortic valve is hypotrophied.
In the second type, the LVOT is hypoplastic, long and tubular and the septum is thickened. The valve, which is situated distally to the membrane, is hypoplastic and incompetent in > 50% of cases, since stenosis reduces the flow from birth and the post-stenotic jet causes trauma to the cusps. This phenomenon requires surgery to be performed early in the course of the disease to protect the aortic valve, i.e. as soon as the mean gradient is > 30 mmHg [5]. It is commonly associated with coarctation of the aorta or a VSD.
Stenosis may also be dynamic and function in the same way as hypertrophic obstructive cardiomyopathy (HOCM). This is characterised by velocity > 2.5 m/s (norm: 1.0-1.5 m/s) and a maximum gradient > 25 mmHg in the LVOT, and is exacerbated by beta sympathetic stimulation, hypovolaemia, and a reduction in peripheral resistance. It is managed by β-amine discontinuation, a β-blocker, hypervolaemia, and an α-stimulant (see Chapter 13 - Dynamic subaortic stenosis). Surgical treatment is indicated if the gradient is > 50 mmHg. It involves resection of the membrane or a myectomy to widen the outflow tract. During surgery, there is a risk of creating a VSD through excessive resection or a persistent gradient through insufficient resection. Perioperative TEE is essential for diagnosing an iatrogenic VSD or an excessive residual gradient. Immediate surgical revision is indicated in 12-35% of cases based on this examination [4,6].
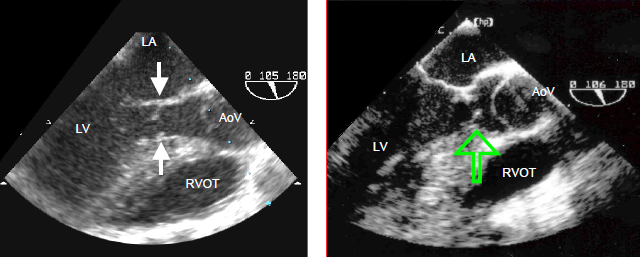
Figure 14.62: TEE image of subaortic stenosis. The arrows indicate the membrane inserted on the septum and on the mitral valve (anterior leaflet).
Bicuspid aortic valve
A bicuspid aortic valve is rarely symptomatic in children [2]. It is often associated with coarctation of the aorta and more rarely with a perimembranous VSD. It can be identified by the presence of two cusps rather than three (Video and Figure 15.49), although cases of unicuspid aortic valve may also be encountered.
Video: Bicuspid aortic valve in a Marfan syndrome; the two leaflets are in an antero-posterior position.
In cases of a stenotic bicuspid aortic valve, surgery is indicated if the mean gradient is ≥ 40 mmHg, area ≤ 0.6 cm2/m2, the patient is symptomatic, or the LV is dilating [5]. In the event of aortic insufficiency (AI), surgery is indicated based on AI severity and LV dilation. In children, implantation of a prosthetic valve is avoided as mechanical prostheses require lifelong anticoagulation and biological prostheses only last 10 to 15 years (see Chapter 11 - Prosthetic Valves). If the valve is flexible, non-calcified and free of insufficiency, the obstacle may be removed and ventricular remodelling prevented by using percutaneous balloon valvotomy. However, there is a risk of creating residual insufficiency. The long-term success rate is 75% at 35 years with a surgical mortality rate of 2.5% [1].
If a valvotomy or reconstruction is inappropriate given the specific circumstances, the pulmonary valve may be transposed to the aortic position (with reimplantation of the coronary arteries) and a homograft implanted in the pulmonary position (Ross procedure) (Figure 14.63). This technique eliminates the need to implant a mechanical prosthesis during growth and suppresses anticoagulation. The reason for this crossing is that homografts degenerate more slowly in a low-pressure system, although their rate of wear is high (30% at 10 years). Moreover, an incompetence in the pulmonary artery root is easier to manage since the right heart can accommodate major variations in volume; on the other hand, stenosis can be dilated by catheterisation without any risk of systemic embolism. The same wear-related lesions in the aortic position would require the implantation of a prosthesis. This operation is contraindicated in the event of pulmonary insufficiency, a bicuspid pulmonary valve, or major ventricular dysfunction. The surgical mortality rate for the Ross procedure is 3% and long-term mortality is < 1%/year. While the deterioration rate for the aortic autograft is 1%/year, it is higher for the homograft on the right outflow tract (2-3%/year). The neoaortic valve becomes insufficient in 30% of patients [3]. The reoperation rate above the age of 12 years is 10% for the aortic valve and 20-30% for the pulmonary homograft [7].
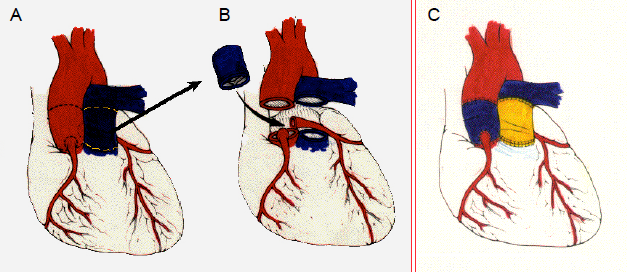
Figure 14.63 Ross procedure This entails resecting the healthy pulmonary valve (A) and the diseased aortic valve (B), and implanting the patient’s pulmonary valve in the aortic position. The pulmonary valve is replaced by a valved conduit between the RV and PA (C). The coronary arteries are reimplanted in the neoaorta.
Supravalvular stenosis
Aortic root narrowing presents as a diaphragm or hourglass deformity. It is located at the sinotubular junction or beyond the sinuses of Valsalva. Consequently, the coronary arteries are upstream of the stenosis and subjected to systolic hypertension. This situation causes these vessels to dilate, speeds up their atheromatous degeneration, and requires surgery to be performed early in the course of the disease. Surgery consists of repairing the aortic root with a widening patch. This is indicated if the mean pressure gradient is ≥ 50 mmHg or the child is symptomatic [5].
Anaesthesia
The constraints applicable to anaesthesia are the same as those for aortic stenosis (see Chapter 11 - Aortic Stenosis, Anaesthesia).
There are two types of fixed subaortic stenosis. The first involves a roughly circular membrane surrounding the outflow tract from the interventricular septum to the anterior leaflet of the mitral valve, and causes the equivalent of aortic stenosis (Video and Figure 14.62).
Video: Long-axis view of a membranous sub-aortic stenosis, visible as a fibrous crest on the septal wall of the left ventricular outflow tract; the aortic valve is hypotrophied.
In the second type, the LVOT is hypoplastic, long and tubular and the septum is thickened. The valve, which is situated distally to the membrane, is hypoplastic and incompetent in > 50% of cases, since stenosis reduces the flow from birth and the post-stenotic jet causes trauma to the cusps. This phenomenon requires surgery to be performed early in the course of the disease to protect the aortic valve, i.e. as soon as the mean gradient is > 30 mmHg [5]. It is commonly associated with coarctation of the aorta or a VSD.
Stenosis may also be dynamic and function in the same way as hypertrophic obstructive cardiomyopathy (HOCM). This is characterised by velocity > 2.5 m/s (norm: 1.0-1.5 m/s) and a maximum gradient > 25 mmHg in the LVOT, and is exacerbated by beta sympathetic stimulation, hypovolaemia, and a reduction in peripheral resistance. It is managed by β-amine discontinuation, a β-blocker, hypervolaemia, and an α-stimulant (see Chapter 13 - Dynamic subaortic stenosis). Surgical treatment is indicated if the gradient is > 50 mmHg. It involves resection of the membrane or a myectomy to widen the outflow tract. During surgery, there is a risk of creating a VSD through excessive resection or a persistent gradient through insufficient resection. Perioperative TEE is essential for diagnosing an iatrogenic VSD or an excessive residual gradient. Immediate surgical revision is indicated in 12-35% of cases based on this examination [4,6].
Figure 14.62: TEE image of subaortic stenosis. The arrows indicate the membrane inserted on the septum and on the mitral valve (anterior leaflet).
Bicuspid aortic valve
A bicuspid aortic valve is rarely symptomatic in children [2]. It is often associated with coarctation of the aorta and more rarely with a perimembranous VSD. It can be identified by the presence of two cusps rather than three (Video and Figure 15.49), although cases of unicuspid aortic valve may also be encountered.
Video: Bicuspid aortic valve in a Marfan syndrome; the two leaflets are in an antero-posterior position.
In cases of a stenotic bicuspid aortic valve, surgery is indicated if the mean gradient is ≥ 40 mmHg, area ≤ 0.6 cm2/m2, the patient is symptomatic, or the LV is dilating [5]. In the event of aortic insufficiency (AI), surgery is indicated based on AI severity and LV dilation. In children, implantation of a prosthetic valve is avoided as mechanical prostheses require lifelong anticoagulation and biological prostheses only last 10 to 15 years (see Chapter 11 - Prosthetic Valves). If the valve is flexible, non-calcified and free of insufficiency, the obstacle may be removed and ventricular remodelling prevented by using percutaneous balloon valvotomy. However, there is a risk of creating residual insufficiency. The long-term success rate is 75% at 35 years with a surgical mortality rate of 2.5% [1].
If a valvotomy or reconstruction is inappropriate given the specific circumstances, the pulmonary valve may be transposed to the aortic position (with reimplantation of the coronary arteries) and a homograft implanted in the pulmonary position (Ross procedure) (Figure 14.63). This technique eliminates the need to implant a mechanical prosthesis during growth and suppresses anticoagulation. The reason for this crossing is that homografts degenerate more slowly in a low-pressure system, although their rate of wear is high (30% at 10 years). Moreover, an incompetence in the pulmonary artery root is easier to manage since the right heart can accommodate major variations in volume; on the other hand, stenosis can be dilated by catheterisation without any risk of systemic embolism. The same wear-related lesions in the aortic position would require the implantation of a prosthesis. This operation is contraindicated in the event of pulmonary insufficiency, a bicuspid pulmonary valve, or major ventricular dysfunction. The surgical mortality rate for the Ross procedure is 3% and long-term mortality is < 1%/year. While the deterioration rate for the aortic autograft is 1%/year, it is higher for the homograft on the right outflow tract (2-3%/year). The neoaortic valve becomes insufficient in 30% of patients [3]. The reoperation rate above the age of 12 years is 10% for the aortic valve and 20-30% for the pulmonary homograft [7].
Figure 14.63 Ross procedure This entails resecting the healthy pulmonary valve (A) and the diseased aortic valve (B), and implanting the patient’s pulmonary valve in the aortic position. The pulmonary valve is replaced by a valved conduit between the RV and PA (C). The coronary arteries are reimplanted in the neoaorta.
Supravalvular stenosis
Aortic root narrowing presents as a diaphragm or hourglass deformity. It is located at the sinotubular junction or beyond the sinuses of Valsalva. Consequently, the coronary arteries are upstream of the stenosis and subjected to systolic hypertension. This situation causes these vessels to dilate, speeds up their atheromatous degeneration, and requires surgery to be performed early in the course of the disease. Surgery consists of repairing the aortic root with a widening patch. This is indicated if the mean pressure gradient is ≥ 50 mmHg or the child is symptomatic [5].
Anaesthesia
The constraints applicable to anaesthesia are the same as those for aortic stenosis (see Chapter 11 - Aortic Stenosis, Anaesthesia).
- Maintain preload (volume).
- Maintain normal heart rate and sinus rhythm – esmolol in cases of tachycardia.
- Maintain systemic perfusion pressure with arterial vasoconstrictors.
- Manage any LV dysfunction.
- In summary, the patient must be: full - regular - vasoconstricted.
Since children are medium-aged, intravenous induction is possible: etomidate (severe cases) or propofol (risk of hypotension). Anaesthesia is performed with fentanyl (10-25 mcg/kg) or sufentanil (0.5-2.5 mcg/kg) and sevoflurane (1-2%). In cases of supra-aortic stenosis, blood flow is diverted so that it surges into the brachiocephalic trunk where the pressure is higher than in the distal aortic arch. It is therefore important to insert the arterial catheter in a left radial or femoral position. In reconstructions of the aortic root, the catheter position varies depending on the surgical strategy and CPB cannulation.
Post-CPB, a residual gradient of 10-20 mmHg is tolerable. Since the aortic sutures are delicate, it is important to avoid any hypertensive crises. A transient or permanent complete AV block is possible due to the proximity of the AV node and the aortic annulus.
Hypoplastic aortic arch
The aortic arch may be stenosed or interrupted in different locations. This disorder is often combined with other cardiac malformations (VSD, hypoplastic LV) and is common in patients with DiGeorge syndrome. Since the distal circulation is provided by the patent ductus arteriosus, the situation deteriorates rapidly when it closes. Surgical reconstruction must therefore be performed in the first weeks of life. This implies deep hypothermic circulatory arrest in order to remodel the arch.
Several days’ additional time can be gained by infusing prostaglandin to maintain ductus arteriosus patency. Heart failure is biventricular, which entails pressure overload for the LV and pressure and volume overload for the RV. Consequently, anaesthesia is based on fentanyl (50-75 mcg/kg) and midazolam. The insertion site for the arterial catheter depends on individual patients’ specific anatomies, although it should ideally be right radial. When reconstructing the aortic arch, the insertion of a second catheter via the femoral route is indicated. Weaning from CPB is typically linked to ventricular failure requiring inotropic support, and to a high risk of haemorrhage.
Shone’s syndrome
Shone's syndrome is characterised by a parachute mitral valve (see Mitral Valve Anomalies), a supravalvular mitral annulus, sub-aortic stenosis, and coarctation of the aorta. Anaesthetic constraints for the dominant lesion apply, i.e. for the lesion that is most upstream and most restrictive for the left-sided flow.
Post-CPB, a residual gradient of 10-20 mmHg is tolerable. Since the aortic sutures are delicate, it is important to avoid any hypertensive crises. A transient or permanent complete AV block is possible due to the proximity of the AV node and the aortic annulus.
Hypoplastic aortic arch
The aortic arch may be stenosed or interrupted in different locations. This disorder is often combined with other cardiac malformations (VSD, hypoplastic LV) and is common in patients with DiGeorge syndrome. Since the distal circulation is provided by the patent ductus arteriosus, the situation deteriorates rapidly when it closes. Surgical reconstruction must therefore be performed in the first weeks of life. This implies deep hypothermic circulatory arrest in order to remodel the arch.
Several days’ additional time can be gained by infusing prostaglandin to maintain ductus arteriosus patency. Heart failure is biventricular, which entails pressure overload for the LV and pressure and volume overload for the RV. Consequently, anaesthesia is based on fentanyl (50-75 mcg/kg) and midazolam. The insertion site for the arterial catheter depends on individual patients’ specific anatomies, although it should ideally be right radial. When reconstructing the aortic arch, the insertion of a second catheter via the femoral route is indicated. Weaning from CPB is typically linked to ventricular failure requiring inotropic support, and to a high risk of haemorrhage.
Shone’s syndrome
Shone's syndrome is characterised by a parachute mitral valve (see Mitral Valve Anomalies), a supravalvular mitral annulus, sub-aortic stenosis, and coarctation of the aorta. Anaesthetic constraints for the dominant lesion apply, i.e. for the lesion that is most upstream and most restrictive for the left-sided flow.
| Anomalies of the left ejection pathway |
|
Three congenital disorders:
- Membranous sub-aortic stenosis (high incidence of valvular dysplasia and AI) - Bicuspid valve (stenosis and/or insufficiency); - Supra-aortic stenosis. Anaesthetic management is the same as for aortic stenosis: Full - Regular - Tight. |
© BETTEX D, BOEGLI Y, CHASSOT PG, June 2008, last update February 2020
References
- DETTER C, FISCHLEIN T, FELDMEIER C, et al. Aortic valvotomy for congenital valvular aortic stenosis. Ann Thorac Surg 2001; 715:1564-71
- FRIEDMAN WF. Aortic stenosis. In: EMMANOULIDES GC, ed. Moss and Adam's heart disease in infants, children and adolescents including fetus and young adult. Baltimore, Williams & Wilkins 1995, p 1087
- FRIGIOLA A, RANUCCI M, CARLUCCI C, et al. The Ross procedure in adults: long-term follow-up and echocardiographic changes leading to pulmonary autograft reoperation. Ann Thorac Surg 2008; 86:482-9
- ROSENFELD HM, GENTLES TL, WERNKOVSKY G, et al. Utility of intraoperative echocardiography in the assessment of residual cardiac defects. Ped Cardiol 1998; 19:346-51
- SILVERSIDES CK, KIESS M, BEAUCHESNE L, et al. Canadian Cardiovascular Society 2009 Consensus Conference on the management of adults with congenital heart disease: Outflow tract obstruction, coarctation of the aorta, tetralogy of Fallot, Ebstein anomaly and Marfan’s syndrome. Can J Cardiol 2010; 26:e80-e97
- STEVENSON JG, SORENSEN GK, GARTMAN DM, et al. Left ventricular outflow tract obstruction: An indication for intraoperative transesophageal echocardiography. J Am Soc Echocardiogr 1993; 6:525-35
- TAKKENBERG JJM, KLIEVERIK LMA, SCHOOF PH, et al. The Ross procedure: a systematic review and meta-analysis. Circulation 2009; 119:222-8