The early correction of tetralogy of Fallot (TOF) during the first year of life allows a survival rate of 80% at 30 years, which makes TOF the third most commonly observed congenital heart disease in adults (9% of cases) and the most common cause of cyanosis [25]. It is caused by the underdevelopment of the right infundibulum. The embryonic parietal band is misaligned and abnormally positioned resulting in obstruction of the right ventricular outflow tract and a wide subaortic VSD [14,26]. The malformation combines four anomalies (Figure 15.38, Figure 15.39 and Figure 15.40) (Videos).
Video: Membranous VSD located under the aortic valve in a case of tetralogy of Fallot.
Video: Long-axis view of the aorta overriding a membranous VSD in a case of tetralogy of Fallot; the right ventricle is severely hypertrophied.
Video: Long-axis view of the right outflow tract in a tetralogy of Fallot; the right ventricular outflow tract is hypertrophied, its lumen is very narrow; the pulmonary valve and artery are hypoplastic.
Video: Membranous VSD located under the aortic valve in a case of tetralogy of Fallot.
Video: Long-axis view of the aorta overriding a membranous VSD in a case of tetralogy of Fallot; the right ventricle is severely hypertrophied.
Video: Long-axis view of the right outflow tract in a tetralogy of Fallot; the right ventricular outflow tract is hypertrophied, its lumen is very narrow; the pulmonary valve and artery are hypoplastic.
- Subaortic VSD (membranous septum);
- Aorta overriding both ventricles;
- Composite stenosis of the right ventricular outflow tract, pulmonary valve, and pulmonary artery;
- Concentric RV hypertrophy.
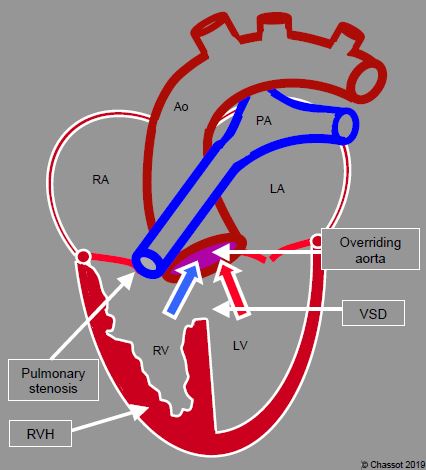
Figure 15.38: Diagram of tetralogy of Fallot, which comprises 4 anomalies: the aortic valve overrides (1) a wide perimembranous VSD (2), the pulmonary valve and artery are stenosed (3) and the RV is hypertrophied (4). The aorta receives a mixture of arterialised blood from the LV and venous blood from the RV through the VSD.
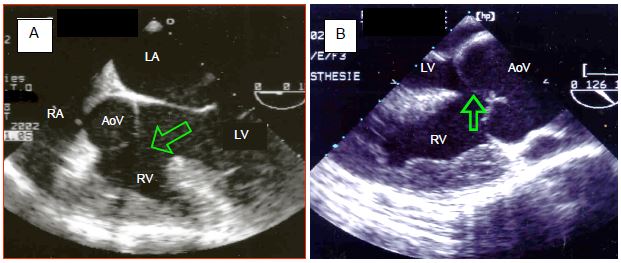
Figure 15.39: Transesophageal echocardiographic images of tetralogy of Fallot. A: 5-chamber view at 0° of the aorta opening in an overriding position over both ventricles. The arrow shows the VSD. The aortic valve receives blood from the LV and RV. The RV is hypertrophied. B: long-axis view at 120° of the aortic root. The valve overrides the VSD (arrow). The RV wall is > 1.2 cm thick and its trabeculations are hypertrophied.
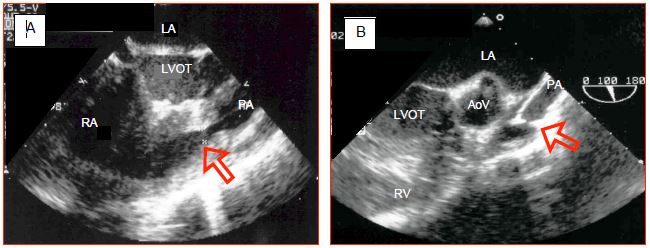
Figure 15.40: Long-axis TEE images at 100-120° of tetralogy of Fallot. A: pulmonary muscular stenosis in the right outflow tract; diameter 0.44 cm (arrow); the pulmonary valve and artery are hypoplastic. B: atresia of the pulmonary valve, whose opening is minuscule (arrow) followed by a hypoplastic and tubular pulmonary artery.
The pulmonary stenosis comprises three components, each of variable severity depending on the case [25].
- Narrowing of the right ventricular outflow tract (RVOT), which is of a dynamic type since this part is entirely muscular (Video). Any increase in contractility or reduction in preload reduces the RVOT diameter, intensifies stenosis and impedes pulmonary flow. Sympathetic stimulation exacerbates cyanosis and therefore these patients are often administered beta-blockers. A membrane is sometimes encountered in the RVOT.
- Small, restrictive, sometimes bicuspid or monocuspid pulmonary valve imposing fixed stenosis (ΔP 50-65 mmHg).
- Hypoplastic pulmonary artery trunk.
Video: Long-axis view of the right outflow tract in a tetralogy of Fallot; the right ventricular outflow tract is hypertrophied, its lumen is minimal with colour flow; the pulmonary valve and artery are hypoplastic..
Patients are cyanotic because pulmonary flow is limited by the stenosis. Most of the blood ejected by the RV flows into the aorta through the VSD. Here, it mixes with arterialised blood from the LV. The pulmonary stenosis protects the lungs against hypertension. If systemic vascular resistance (SVR) increases, the proportion of arterialised blood received by the aorta increases since the R-to-L component of the shunt decreases. This mechanism is used in squatting position [25]. Since the RV is subjected to systemic pressure, it is hypertrophied, but gradually dysfunctions and, without correction, ultimately fails. The aortic valve is competent in children, but gradually dilates over the years to the extent that aortic insufficiency (grade 1-2) is present in 75% of adults (Figure 15.41) (Video) [15].
Video: Aortic regurgitation in a tetralogy of Fallot.
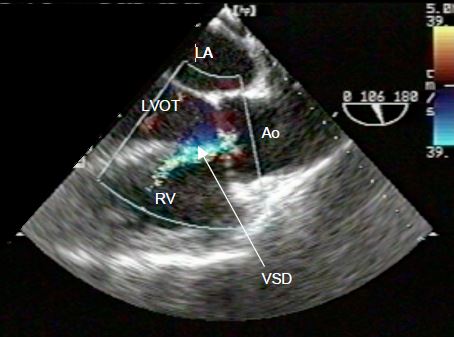
Figure 15.41: TEE image of tetralogy of Fallot. Aortic insufficiency (colour jet) overriding the VSD in an unoperated adult.
In some cases, an ASD is added to the other lesions, which is described as pentalogy. Several lesions may be associated with TOF such as a right-sided aortic arch or coronary artery anomalies (10% of cases) [20]. Arrhythmias are common: atrial tachycardia (30% of cases), ventricular tachyarrhythmia linked to the degree of RV dilation (10% of cases). The incidence of sudden death is 0.2% per year [27].
Patients are cyanotic and present with clubbing of the fingers. Auscultation reveals a grade 3/6 systolic murmur accompanied by a systolic thrill at the left sternal border towards the second or third intercostal space. A medium-frequency mid-diastolic murmur at the same location is typical of pulmonary insufficiency. The survival rate among unoperated patients is 30% at 10 years, but under 3% among those aged over 40 years [2]. Their survival is dependent on vicariance of pulmonary blood flow through collateral arteries stemming from the bronchial arteries. These collaterals sometimes maintain sufficient pulmonary blood flow for patients to reach adulthood without cyanosis (Figure 15.42). In such cases, systemic diastolic pressure is low, since blood from the thoracic aorta escapes into the low-pressure pulmonary circuit during diastole. Unfortunately, this remains a precarious situation, since the LV must supply the systemic and pulmonary blood flow simultaneously, leading to its gradual failure.
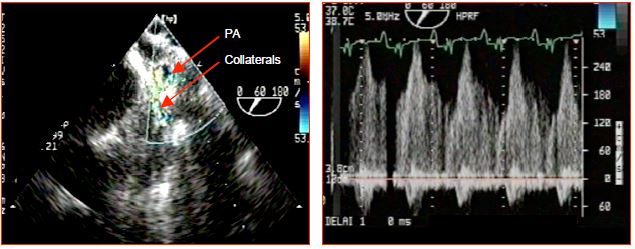
Figure 15.42: Collateral flow in a case of tetralogy of Fallot. The flow is visible between a large collateral originating from the descending aorta and a branch of the pulmonary artery (PA). It is a continuous systolic and diastolic flow, since systemic pressure is constantly higher than pulmonary pressure. If sufficient in number, these collaterals may ensure normal pulmonary blood flow at rest.
There is a whole range of lesions similar to those of TOF. Ten percent of all congenital heart disease patients experience some degree of pulmonary stenosis (see Pulmonary stenosis) [13]. Their anatomy is similar to Fallot cases, although without a VSD or displacement of the aorta. They are not cyanotic at rest. Such cases are sometimes described as pink Fallot.
The echocardiographic image is distinctive [3,16]. The aortic valve is very large and overrides a VSD, which opens onto both ventricles (Vidéo Fallot CIV). Blood flows into the aorta from the LV and the RV without any genuine shunting occurring between the two ventricles. A narrow and highly accelerated flow can be identified in the RVOT, whose musculature is hypertrophied (Vidéo Fallot St pulm coul). Pulmonary stenosis may also involve a subpulmonary membrane and/or hypoplastic pulmonary valve, which may be bicuspid. The pulmonary vascular tree is hypoplastic to a variable degree (Vidéo Fallot st pulm). Normally, maximum pulmonary velocity (approximately 3-4 m/s, corresponding to a pressure gradient of 35-65 mmHg) exhibits an early systolic peak in the event of fibrotic stenosis, but an end systolic peak in the event of dynamic muscular stenosis. Aortopulmonary collaterals appear as continuous, turbulent systolic and diastolic flows located in the posterior mediastinum (Vmax 2-3 m/s). Sometimes, it is possible to trace them between the aorta and a pulmonary artery (Video).
Video: Collateral between the systemic and pulmonary circulation in the posterior mediastinum; the flow is continuous systolo-diastolic.
Surgery
In the nineteen seventies, two-stage surgery was generally performed on these patients. A L-to-R shunt was first performed to increase pulmonary blood flow: Blalock-Taussig shunt (subclavian artery → right or left pulmonary artery), Potts shunt (descending aorta → left PA) or Waterston shunt (ascending aorta → right PA). The shunt’s size determined its flow rate; the arterial saturation was reaching 80-85%. This initial surgical procedure was followed by total correction between the ages of 5 and 10 years. Unfortunately, this strategy maintained hypoxia and pressure overload on the RV for too many years. It also caused deformity of the pulmonary arteries.
Currently, total correction is performed in early childhood (between 3 and 18 months), which eliminates cyanosis, normalises pulmonary blood flow and encourages growth of the pulmonary vascular tree [7,19]. The operation entails occluding the VSD with a patch or by direct closure with realignment of the septum, and enlarging the right ventricular outflow tract and the pulmonary valve, either with or without a patch. A valved conduit may also be inserted between the RV and PA (Figure 15.43).
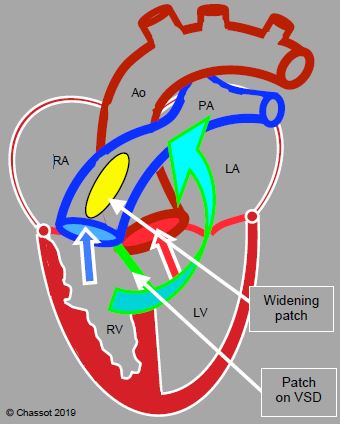
Figure 15.43: Surgical correction of tetralogy of Fallot. The VSD patch divides the flows, guiding systemic venous blood to the PA and arterialised blood to the aorta. A patch enlarging the RVOT and pulmonary valve removes the pulmonary and subpulmonary stenosis. The arrow shows the point at which a valved conduit may be inserted between the RV and PA if a patch is not feasible.
Enlargement of the RVOT entails a risk of pulmonary insufficiency if the patch is too large or of persistent stenosis if it is too restrictive. Correction is therefore based on a compromise between minimal regurgitation and minimal residual gradient. The maximum accepted gradient is 20-30 mmHg [30]. A flow rate of > 3 m/s or a gradient of > 40 mmHg are considered excessive. When resecting a dynamic hypertrophy of the outflow tract, the residual gradient may be functional rather than anatomical. It is reduced by decreasing sympathetic tone and raising loading conditions. The surgical mortality rate for total correction performed at an early age is < 2% and the survival rate is ≥ 92% at 30 years [8,18,27]. Most children who undergo surgery at 3-12 months require a second operation due to pulmonary insufficiency or stenosis or in order to implant a wider conduit, whereas only 10-15% of patients who undergo surgery in adulthood require subsequent reoperation [21].
Correction may leave a number of major sequelae [12].
- Arrhythmias: right bundle branch block or bifascicular block (50% of cases), premature ventricular contraction, AF, sudden death (40% of long-term causes of death). To reduce the risk of arrhythmia, the transatrial or transpulmonary approach is practised, avoiding incisions to the ventricle wall or RVOT [23]. Arrhythmias are directly linked to the degree of RV dilation.
- Residual VSD (10-20%).
- Pulmonary insufficiency (PI) with RV dilation.
- Residual stenosis of the pulmonary conduit or RVOT.
- Residual stenosis on the peripheral pulmonary arteries.
- Dilation of the aortic root (≥ 60 mm) and aortic insufficiency.
The degree of postoperative PI is a significant prognostic factor for subsequent right ventricular function. While PI is generally well tolerated, if it is severe (Grade 3-4), the RV dilates significantly and dysfunctions (Figure 15.44) (Video). Major tricuspid insufficiency becomes established; the risk of tachyarrhythmia is high. The pulmonary valve must be replaced sufficiently early to prevent right-sided complications [6,22].
Video: Dilatative hypertrophy of the right ventricle in a case of Fallot operated in childhood and presenting a severe pulmonary regurgitation in adulthood.
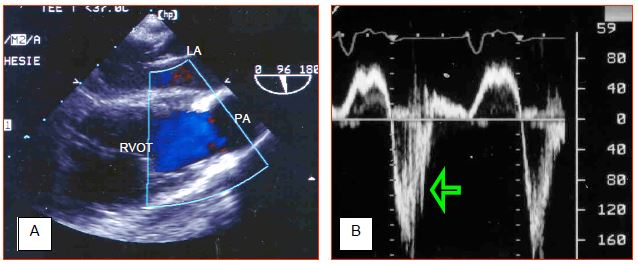
Figure 15.44: Severe pulmonary insufficiency several years after correction of tetralogy of Fallot. A: long-axis view of the right ventricular outflow tract (RVOT) and the root of the pulmonary artery (PA). The pulmonary valve is non-existent, diastolic reflux occupies the conduit's full diameter and does not exhibit any turbulence as pressure equalises immediately between the PA and RV during diastole. B: blood flow in the PA root – there is significant diastolic reflux (arrow). The area under the curve and velocity time integral (VTI) of the diastolic component are greater than those of the systolic component. However, the stroke volume is the product of VTI and the vessel section area. Since the pulmonary artery is dilated during systole and its size decreases during diastole due to its pulsatility, this product is higher during systole than during diastole [5].
Surgical correction will not ensure adequate functional recovery of the RV if its size is > 150 mL/m2 [28]. In the event of residual stenosis of the RVOT, the RV is subjected to pressure overload. A RV/LV pressure ratio > 0.6 is poorly tolerated in the long term and the ventricle fails (Figure 15.45) (Video).
Video: Hypertrophy and dysfunction of the right ventricle in a case of Fallot operated in childhood and presenting a severe pulmonary stenosis in adulthood.
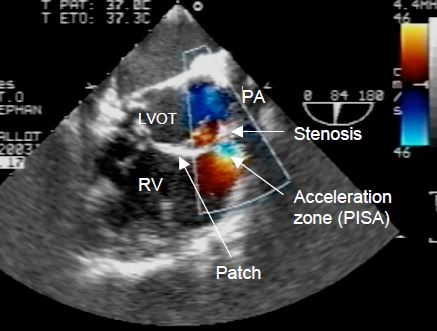
Figure 15.45: Pulmonary stenosis after surgical correction of TOF. Eighteen years after surgery, the RV (in the centre of the image) is hypertrophied and dilated due to the residual stenosis of the pulmonary valve. Blood flow through the significantly reduced pulmonary orifice is accelerated and turbulent. The VSD patch is visible below the aortic valve, between the LVOT and RVOT.
Pulmonary insufficiency and/or stenosis are the main cause of reoperation of Fallot patients in adulthood (15-40% of cases at 20-30 years) [21]. In the event of PI, surgery is indicated if the RV is dilated (EDV ≥ 170 mL/m2), failing or arrhythmic (QRS ≥ 180 ms) [25]. In the event of stenosis, surgery is indicated if the maximum gradient ≥ 50 mmHg and/or the RV/LV pressure ratio ≥ 0.7 [4,29]. In both cases, surgery is indicated if moderate to severe tricuspid insufficiency is present [27]. Reoperation to implant a valved conduit between the RV and PA is generally necessary. Although this protects the right ventricle and impedes the onset of arrhythmias, it does not enable full functional recovery of the RV [1,9,23]. However, right-sided dysfunction is the main predictor of these patients’ survival, especially since the incidence and severity of arrhythmias are directly related to it. Right-sided dysfunction and incomplete or late correction are the main factors increasing the likelihood of arrhythmias and sudden deaths (incidence: 2%/10 years) [11]. LV dysfunction is proportionate to the delay until total correction, the degree of cyanosis, and the period during which pulmonary flow was provided by a palliative shunt (Blalock, Potts, etc.). After correcting a stenosis, there is an important risk of pulmonary reperfusion syndrome, characterized by an acute pulmonary oedema and a massive ARDS [25]. Due to progress made with transcatheter-implantable prostheses (Melody, SAPIEN), a less invasive route for pulmonary valve replacement is possible, provided that there is a sufficiently firm support into which to anchor the prosthesis, e.g. a previous valved conduit [17,27]. The mortality of pulmonary valve replacement is 2% at 5 years, and the risk of reoperation is 5% [25].
Since drug treatment of arrhythmias is ineffective, patients often undergo implantation of a defibrillator within a cardiac chamber, thermo-ablation by catheterisation, or a maze procedure [27].
Anaesthesia in the event of uncorrected TOF
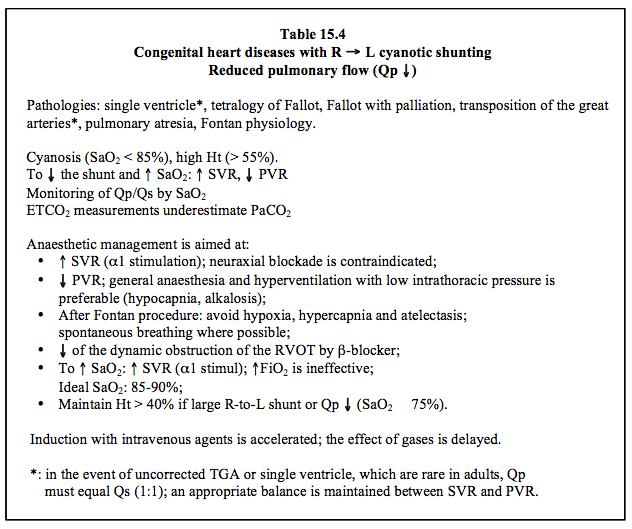
If the malformation is not corrected, the haemodynamic conditions are highly restrictive. Two objectives are pursued: reducing the shunt and increasing pulmonary blood flow (Table 15.4) [25].
Video: Dilatative hypertrophy of the right ventricle in a case of Fallot operated in childhood and presenting a severe pulmonary regurgitation in adulthood.
Figure 15.44: Severe pulmonary insufficiency several years after correction of tetralogy of Fallot. A: long-axis view of the right ventricular outflow tract (RVOT) and the root of the pulmonary artery (PA). The pulmonary valve is non-existent, diastolic reflux occupies the conduit's full diameter and does not exhibit any turbulence as pressure equalises immediately between the PA and RV during diastole. B: blood flow in the PA root – there is significant diastolic reflux (arrow). The area under the curve and velocity time integral (VTI) of the diastolic component are greater than those of the systolic component. However, the stroke volume is the product of VTI and the vessel section area. Since the pulmonary artery is dilated during systole and its size decreases during diastole due to its pulsatility, this product is higher during systole than during diastole [5].
Surgical correction will not ensure adequate functional recovery of the RV if its size is > 150 mL/m2 [28]. In the event of residual stenosis of the RVOT, the RV is subjected to pressure overload. A RV/LV pressure ratio > 0.6 is poorly tolerated in the long term and the ventricle fails (Figure 15.45) (Video).
Video: Hypertrophy and dysfunction of the right ventricle in a case of Fallot operated in childhood and presenting a severe pulmonary stenosis in adulthood.
Figure 15.45: Pulmonary stenosis after surgical correction of TOF. Eighteen years after surgery, the RV (in the centre of the image) is hypertrophied and dilated due to the residual stenosis of the pulmonary valve. Blood flow through the significantly reduced pulmonary orifice is accelerated and turbulent. The VSD patch is visible below the aortic valve, between the LVOT and RVOT.
Pulmonary insufficiency and/or stenosis are the main cause of reoperation of Fallot patients in adulthood (15-40% of cases at 20-30 years) [21]. In the event of PI, surgery is indicated if the RV is dilated (EDV ≥ 170 mL/m2), failing or arrhythmic (QRS ≥ 180 ms) [25]. In the event of stenosis, surgery is indicated if the maximum gradient ≥ 50 mmHg and/or the RV/LV pressure ratio ≥ 0.7 [4,29]. In both cases, surgery is indicated if moderate to severe tricuspid insufficiency is present [27]. Reoperation to implant a valved conduit between the RV and PA is generally necessary. Although this protects the right ventricle and impedes the onset of arrhythmias, it does not enable full functional recovery of the RV [1,9,23]. However, right-sided dysfunction is the main predictor of these patients’ survival, especially since the incidence and severity of arrhythmias are directly related to it. Right-sided dysfunction and incomplete or late correction are the main factors increasing the likelihood of arrhythmias and sudden deaths (incidence: 2%/10 years) [11]. LV dysfunction is proportionate to the delay until total correction, the degree of cyanosis, and the period during which pulmonary flow was provided by a palliative shunt (Blalock, Potts, etc.). After correcting a stenosis, there is an important risk of pulmonary reperfusion syndrome, characterized by an acute pulmonary oedema and a massive ARDS [25]. Due to progress made with transcatheter-implantable prostheses (Melody, SAPIEN), a less invasive route for pulmonary valve replacement is possible, provided that there is a sufficiently firm support into which to anchor the prosthesis, e.g. a previous valved conduit [17,27]. The mortality of pulmonary valve replacement is 2% at 5 years, and the risk of reoperation is 5% [25].
Since drug treatment of arrhythmias is ineffective, patients often undergo implantation of a defibrillator within a cardiac chamber, thermo-ablation by catheterisation, or a maze procedure [27].
Anaesthesia in the event of uncorrected TOF
If the malformation is not corrected, the haemodynamic conditions are highly restrictive. Two objectives are pursued: reducing the shunt and increasing pulmonary blood flow (Table 15.4) [25].
- Increasing systemic arterial resistance – this reduces the cyanotic R-to-L shunt, although at the cost of reducing systemic perfusion if vasoconstriction is intense. Moreover, arterial hypertension increases LV and RV afterload at a time when the RV is already under stress as it is subjected to systemic ejection pressure. SpO2 provides an effective and immediate means of monitoring the extent of shunting (Figure 15.46).
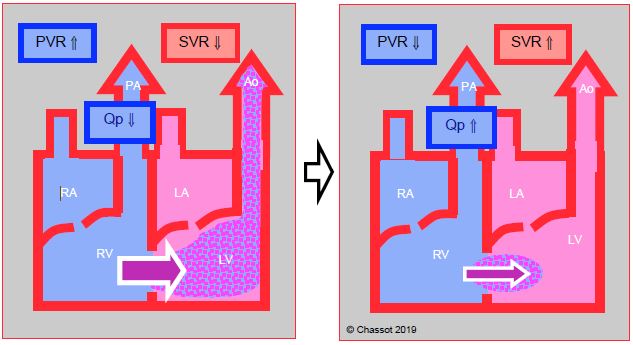
Figure 15.46: Right → left shunt. This is increased when SVR falls, which lowers the pulmonary arterial blood flow (Qp). The shunt is reduced if SVR increases and PVR falls. As a result, pulmonary flow increases and SaO2 improves.
- Increasing pulmonary flow – in the event of a fixed obstruction, arterial vasoconstriction (alpha stimulants) is indicated. However, if the obstruction is dynamic, beta blockade is necessary to relax the RVOT's musculature. In such cases, beta-stimulants are contraindicated.
- Maintaining normovolaemia – in the event of hypovolaemia, the shunt's R-to-L component increases, for instance if systemic pressure falls.
- Restricting the situations where PVR raise and increase the R-to-L component of the shunt (hypoxia, hypercapnia, stress, pain); insure hyperventilation and adequate sedation (midazolam, dexmedetomidine).
- Neuraxial blockade lowers preload and SVR, which is doubly detrimental. Only an epidural with very gradual installation of sympathetic blockade and strict monitoring of haemodynamics is appropriate.
If palliation by means of a simple systemic → pulmonary shunt is in place, pulmonary perfusion is dependent on satisfactory systemic pressure. Any arterial vasodilation lowers the shunt flow, thereby also reducing pulmonary flow – cyanosis increases. Moreover, hypotension incurs a risk of coronary ischaemia. These patients therefore also benefit from increased SVR (Figure 15.47). Diastolic arterial pressure is chronically lowered if the shunt is flowing satisfactorily, since pressure in the pulmonary vascular tree is very low. Since the LV must ensure systemic and pulmonary perfusion, it functions at volume overload and bordering on failure. The same is true of patients who have survived to adulthood due to a highly developed network of collaterals linking the thoracic aorta to the pulmonary vascular tree.
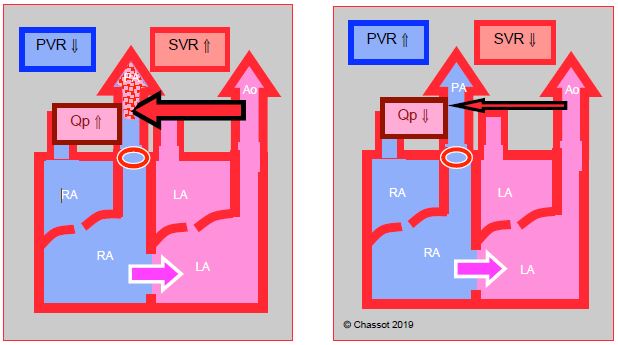
Figure 15.47: Left → right corrective shunt to increase pulmonary blood flow (Qp) in the event of pulmonary stenosis. Its blood flow diminishes as SVR falls and also rises as SVR increases.
Anaesthesia in the event of corrected TOF
The earlier correction is performed, the better the function of both ventricles is preserved. Nevertheless, arrhythmias are common under all circumstances [10].
- Right ventricle: in the event of pulmonary insufficiency through the patched area, the RV dilates and fails due to volume overload. It is therefore imperative to avoid anything that increases its afterload and also to induce pulmonary vasodilation (normobaric hyperventilation, alkalosis, prostaglandin, etc.). In the event of pressure overload (PRV / PLV > 0.5), adequate coronary perfusion pressure and a normal heart rate must be maintained due to the risk of subendocardial ischaemia of the RV. In both cases, a vasopressor (norepinephrin) and inotropic support (dobutamine, milrinone) are usually required.
- Left ventricle: its overload is linked to collaterals supplying the pulmonary network.
- Arrhythmias: bundle branch blocks (usually right-sided) in 50% of cases, atrial tachycardia (30% of cases) ventricular tachyarrhythmia in 10% of cases. A prophylactic pacemaker may be indicated.
- Arterial pressure measurement in the arm opposite the side of the palliative shunt.
| Tetralogy of Fallot (TOF) |
| Characteristics: - Subaortic VSD (membranous septum); - Aorta overriding the VSD - Pulmonary stenosis (RVOT, pulmonary valve, PA trunk) - RVH (RV connected to systemic pressure) Cyanotic R → L shunt, reduced pulmonary blood flow (Qp ↓, Qp/Qs < 1.0) In order to reduce the shunt, increase SVR (alpha stimulation) and reduce PVR (hyperventilation). If dynamic component (RVOT): beta-blocker SaO2 proportionate to Qp/Qs Anaesthesia recommendations: - Sevoflurane or midazolam/propofol GA - Ventilation: hypocapnia, FiO2 has no significant effect on SpO2 - Increase SVR to ↑ SpO2 - Avoid systemic vasodilation - Maintain preload: hypovolaemia increases cyanotic R → L shunting - Spinal anaesthesia inappropriate – if neuraxial blockade: epidural with gradual installation of sympathetic blockade If pulmonary blood flow is ensured by a palliative shunt (e.g. Blalock-Taussig) or Ao →PA collaterals (fixed flow): - Qp proportionate to systemic AP - Keep SVR ↑ - Hypovolaemia/hypotension: Qp ↓, cyanosis ↑ After surgical correction: - Sequelae: pulmonary stenosis or insufficiency - Arrhythmias - RV dysfunction - Dilation of the aortic root and AI - LV dysfunction |
© BETTEX D, CHASSOT PG, January 2008, last update February 2020
References
- BAUMGARTNER H, BONHOEFFER P, DE GROOT NMS, et al. ESC Guidelines for the management of grown-up congenital heart disease (new version 2010). Eur Heart J 2010; 31:2915-57
- BERTRANOU EG, BLACKSTONE EH, HAZELRIG JB, et al. Life expectancy without surgery in tetralogy of Fallot. Am J Cardiol 1978; 42:458-66
- BETTEX D, CHASSOT PG. Malformations congénitales de l'adulte. In: BETTEX D, CHASSOT PG. Echocardiographie transoesophagienne en anesthésie – réanimation. Paris: Pradel-Masson, Williams & Wilkins, 1997, 171-87
- BHATT AB, FOSTER E, KUEHL K, et al. Congenital hesart disease in older adult. A Scientific Statement from the American Heart Association. Circulation 2015; 131:1884-931
- CHASSOT PG, BETTEX D. Perioperative transoesophageal echocardiography in adult congenital heart disease. In: POELAERT J, SKARVAN K. Transoesophageal echocardiography in anaesthesia. London, BMJ Book, 2004
- DAVLOUROS PA, NIWA K, WEBB G, GATZOULIS MA. The right ventricle in congenital heart disease. Heart 2006; 92(Suppl 1): i27-i38
- DIDONATO RM, JONAS RA, LANG P, ROWE JJ, CASTANEDA AR. Neonatal repair of tetralogy of Fallot with and without pulmonary atresia. J Thorac Cardiovasc Surg 1991; 101:126-37
- ERIKSSEN G, LIESTOL K, SEEM E, et al. Achievements in congenital heart defect surgery: a prospective, 40-year study of 7'038 patients. Circulation 2015; 131:337-46
- EYSKENS B, REYBROUCK T, BOGAERT J, et al. Homograft insertion for pulmonary regurgitation after repair of tetralogy of Fallot improves cardiorespiratory performance. Am J Cardiol 2000; 85:221-5
- FINDLOW D, DOYLE E. Congenital heart disease in adults. Br J Anaesth 1997; 78:416-30
- GATZOULIS MA, BALAJI S, WEBBER SA, et al. Risk factors for arrhythmia and sudden cardiac death late after repair of tetralogy of Fallot: a multicentre study. Lancet 2000; 356:975-81
- JIMENEZ M, ESPILl G, THAMBO JB, et al: Outcome of operated Fallot's tetralogy. Arch Mal Coeur Vaiss 2002; 95:1104-11
- KAPLAN J, ADOLPH RJ. Pulmonary valve stenosis in adults. Cardiovasc Clinics 1979; 10:327-33
- KLOESEL B, DINARDO JA, BODY SC. Cardiac embryology and molecular mechanisms of congenital heart disease – A primer for anesthesiologists. Anesth Analg 2016; 123:551-69
- MARELLI AJ, PERLOFF JK, CHILD JS, et al. Pulmonary atresia with ventricular septal defect in adults. Circulation 1994; 89:243-51
- MILLER-HANCE WC, SILVERMAN NH. Transesophageal echocardiography (TEE) in congenital heart disease with focus on the adult. Cardiol Clinics 2000; 18:861-92
- NISHIMURA RA, OTTO C, BONOW RO, et al. 2014 AHA/ACC Guideline for the management of patients with valvular heart disease. A report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. Circulation 2014; 129:e521-e643
- NOLLERT G, FISCHLEIN T, BOUTEWERK S, et al. Long-term survival in patients with repair of tetralogy of Fallot: 36 year follow-up of 490 survivors of the first year after surgical repair. J Am Coll Cardiol 1997; 30:1374-83
- PIGULA FA, KHALIL PN, MAYER JE, et al. Repair of tetralogy of Fallot in neonates and young infants. Circulation 1999; 100(Suppl II):157-61
- ROUINE-RAPP K, RUSSELL IA, FOSTER E. Congenital heart disease in the adult. Int Anesthesiol Clin 2012; 50:16-39
- SILVERSIDES CK, KIESS M, BEAUCHESNE L, et al. Canadian Cardiovascular Society 2009 Consensus Conference on the management of adults with congenital heart disease: Outflow tract obstruction, coarctation of the aorta, tetralogy of Fallot, Ebstein anomaly and Marfan’s syndrome. Can J Cardiol 2010; 26:e80-e97
- STOUT KK, DANIELS CJ, VALENTE AM, et al. 2018 AHA/ACC Guideline for the management of adults with congenital heart disease. J Am Coll Cardiol 2019; 73:e81-192
- SYFRIDIS PG, KIRVASSILIS GV, PAPAGIANNIS JK, et al. Preservation of right ventricular structure and function following transatrial-transpulmonary repair of tetralogy of Fallot. Eur J CardioThor Surg 2013; 43:336-42
- THERRIEN J, SIU SC, HARRIS L, et al. Impact of pulmonary valve replacement on arrythmia propensity late after repair of tetralogy of Fallot. Circulation 2001; 103:2489-94
- TOWNSLEY MM, WINDSOR J, BRISTON D, et al. Tetralogy of Fallot: perioperative management and analysis of outcomes. J Cardiothorac Vasc Anesth 2019; 33:556-65
- VAN PRAAGH R. Tetralogy of Fallot: underdevelopment of the pulmonary infundibulum and its sequelae. Am J Cardiol 1970; 47:1279
- VILLAFAÑE J, FEINSTEIN JA, JENKINS KJ, et al. Hot topics in tetralogy of Fallot. J Am Coll Cardiol 2013; 62:2155-66
- WARNES CA. Adult congenital heart disease. Importance of the right ventricle. J Am Coll Cardiol 2009; 54:1903-10
- WARNES CA, WILLIAMS RG, BASHORE TM, et al. ACC/AHA 2008 Guidelines for the management of adults with congenital heart disease: executive summary. Circulation 2008; 118:2395-451
- WEINTRAUB R, SHIOTA T, ELKADI T, et al. Transesophageal echocardiography in infants and children with congenital heart disease. Circulation 1992; 86:711-22