- If stenosis predominates, the LA is huge and the ventricle disproportionately small; spontaneous contrast is often absent as a result of mixing in the LA by the MI. The interatrial septum permanently bulges into the ventricle.
- If the insufficiency is predominant, the LV is dilated and hypertrophied; the LA is less voluminous, the interatrial septum bulges into the RV only in systole.
The volume regurgitated in systole increases the volume that must pass through the valve in diastole. This excess increases the gradient and leads to an overestimation of the degree of stenosis by the half-pressure time measurement. On the other hand, the combination of MI and MS keeps LV dimensions in the intermediate range and limits ventricular remodelling: the presence of MI reduces the risk of LV hypotrophy and the presence of MS reduces the risk of dilatation. This is particularly beneficial in patients weaning off ECC. However, the degree of haemodynamic disturbance is greater than for the same degree of severity in isolated pathology; therefore, the indication for surgery is generally based on the patient's symptoms during exercise rather than on calculated values [2].
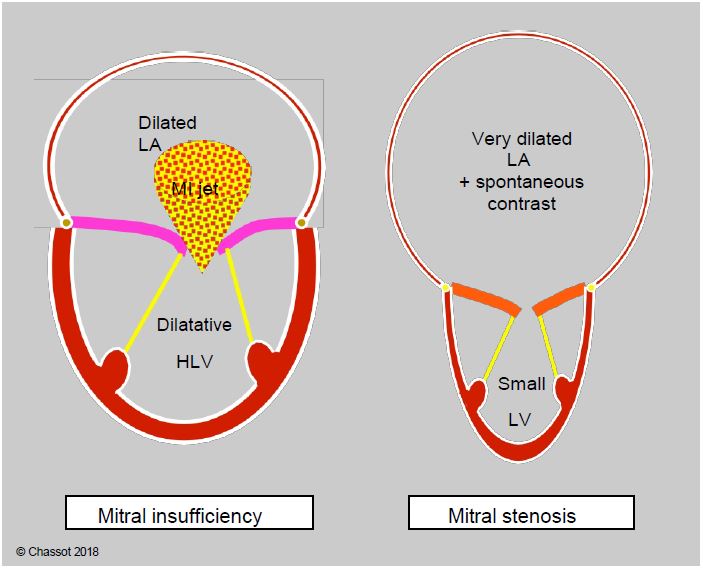
Figure 11.99: Comparative silhouettes of mitral regurgitation and stenosis. In the combination of the two conditions characteristic of mitral disease, the predominant condition is clearly identified by the general appearance of the left cavities.
| Hemodynamics sought in mitral valve disease |
| High preload RAS ↑ if stenosis predominates, RAS ↓ if insufficiency predominates Normal rate Maintain sinus rhythm Inotropic support in ventricular dysfunction (Dts > 2.5 cm/m2, Dtd > 4 cm/m2) Pulmonary vasodilatation (PAR↓) Well tolerated positive ventilation |
© CHASSOT PG, BETTEX D, August 2011, last update November 2019
References
- NISHIMURA RA, OTTO CM, BONOW RO, et al. 2014 AHA/ACC Guideline for the Management of Patients with Valvular Heart Disease. Circulation 2014; 129:e521-e643
- UNGER P, CLAVEL MA, LINDMAN BR, et al. Pathophysiology and management of multivalvular heart disease. Nat Rev Cardiol 2016; 13:429-40