The surface area of the tricuspid valve (7-9 cm2) is about 20% greater than that of the mitral valve. Its three leaflets are thin (< 1 mm thick) and unequal in size: the anterior leaflet is the largest, the posterior leaflet is of medium size and the septal leaflet is the smallest and most restrictive; its septal insertion is 10 mm more apical than that of the anterior mitral leaflet; some of its chords are anchored directly to the interventricular septum and limit its movements. The posteroseptal commissure is at the level of the coronary sinus. The tricuspid valve has 3 pillars, one of which is on the interventricular septum. The tricuspid annulus fibrosus is incomplete; it does not extend posterolaterally, which is why it enlarges in this direction during dilation (see Figure 11.12). Like the mitral annulus, it has a saddle shape with the raised points in the antero-posterior axis and the lower points in the septo-lateral axis, but unlike the latter it has an oval silhouette with the long axis in the antero-posterior direction and the wider base at the posterior leaflet (see Figure 11.61). Its surface area decreases by 25% during systole [2,4]. As it dilates, the ring becomes flatter and more circular.
Measured on a 4-chamber echocardiogram, the normal diameter is 2.8 ± 0.5 cm (2.5-3.9 cm) in diastole; dilatation is significant if it is ≥ 4.0 cm (2.1 cm/m2 ) (Figure 11.151) [1,3,4]. Dilatation of the tricuspid annulus and the free wall of the RV leads to tricuspid insufficiency (TI) because the anterior and posterior leaflets are unable to join together in systole (Figure 11.152).
Video: Major tricuspid insufficiency in admission view - 60° RV flap centered on the tricuspid valve
The pressure gradient across the tricuspid valve in diastole is < 2 mmHg (Vmax flow E approximately 0.5 m/s). Tricuspid surgery must avoid two anatomical pitfalls: 1) the anteroseptal commissure is 3-5 mm from the AV node and His bundle, 2) the right coronary artery, located in the atrioventricular groove, is 5 mm from the implantation of the anterior and posterior leaflets.
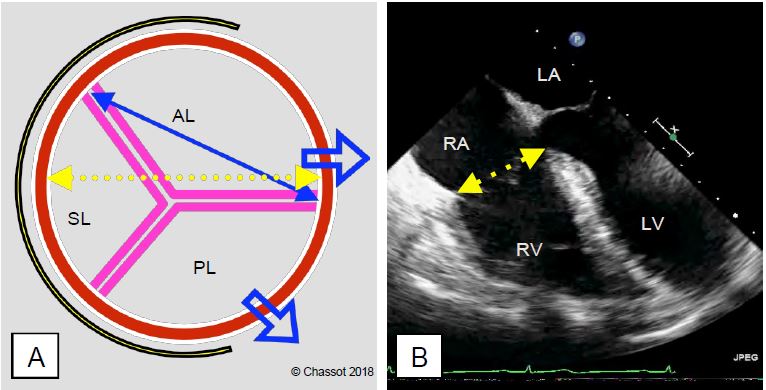
Figure 11.151: Tricuspid valve and tricuspid annulus diameter measurements. A: Diagram of the valve seen from the outside; the septum is to the left of the image. The valve is elliptical. The three leaflets of the tricuspid valve are unequal in size: the anterior leaflet is the largest, the posterior leaflet is of medium size and the septal leaflet is smaller and more restrictive. The tricuspid annulus fibrosus (yellow) is incomplete; it does not extend posterolaterally. On dilation the valve extends posterolaterally (blue arrows) where the annulus fibrosus is interrupted. B: Transoesophageal 4-chamber echocardiogram; normal diameter is 2.8 ± 0.5 cm; dilatation is significant if ≥ 4.0 cm [1]; these two-dimensional images underestimate the true anatomical diameter. In the surgical field, the diameter is measured between the anteroseptal and anteroposterior commissures (double blue arrow in A). In B, the gap of about 1 cm between the septal insertion of the tricuspid valve and that of the mitral valve is clearly visible; it corresponds to the fibrous part of the interventricular septum.
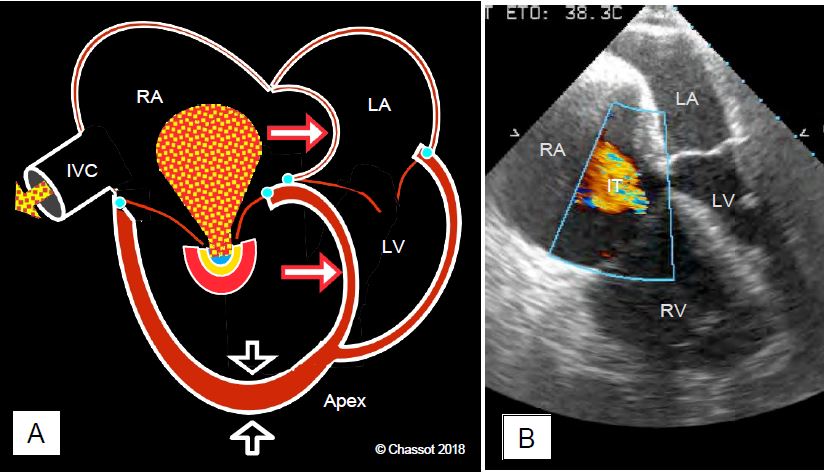
Figure 11.152: Tricuspid regurgitation due to dilatation and dysfunction of the RV. A: The RV is dilated and hypertrophied (RVH); the interventricular septum bulges into the LV and restricts diastolic filling. Dilatation of the tricuspid annulus leads to regurgitation (TI); the RA is dilated and the septum bulges strongly into the LA. The apex of the heart is formed by the RV and not the LV as normal. The IT is severe (PISA on the ventricular surface) and there is systolic reflux into the inferior vena cava. B: 4-cavity TEE view during an episode of acute pulmonary embolism in a patient with an enlarged LV due to chronic pulmonary hypertension.
Transoesophageal echocardiography examines the tricuspid valve in multiple planes (Figure 26.46).
- Mid-oesophageal 4-plane view 0-20°; the standard 4-plane view shows the septal leaflet and a non-septal leaflet, which may be the anterior leaflet in the high position or the posterior leaflet in the low position. The normal diameter of the annulus in telediastole in this view is ≤ 2.1 cm/m2.
- 5-cavity view of the middle oesophagus 0-20° (presence of the aortic valve on the slice); this slightly higher image of the probe cuts the septum and the anterior leaflet.
- Lower oesophagus 4-cavity view 0-20° (the coronary sinus is present in the section); when the probe is in the lower position, the septal and posterior leaflets are visible.
- Intake view - 60° RV inflow tract (anterior and posterior leaflets).
- Transgastric view of the 30-90° RV inflow tract; the only short axis view of the valve where all 3 leaflets are visible; this image is sometimes difficult to obtain.
- Transgastric view of the 90-130° RV inflow tract (anterior and posterior leaflets); this view clearly shows the subvalvular apparatus.
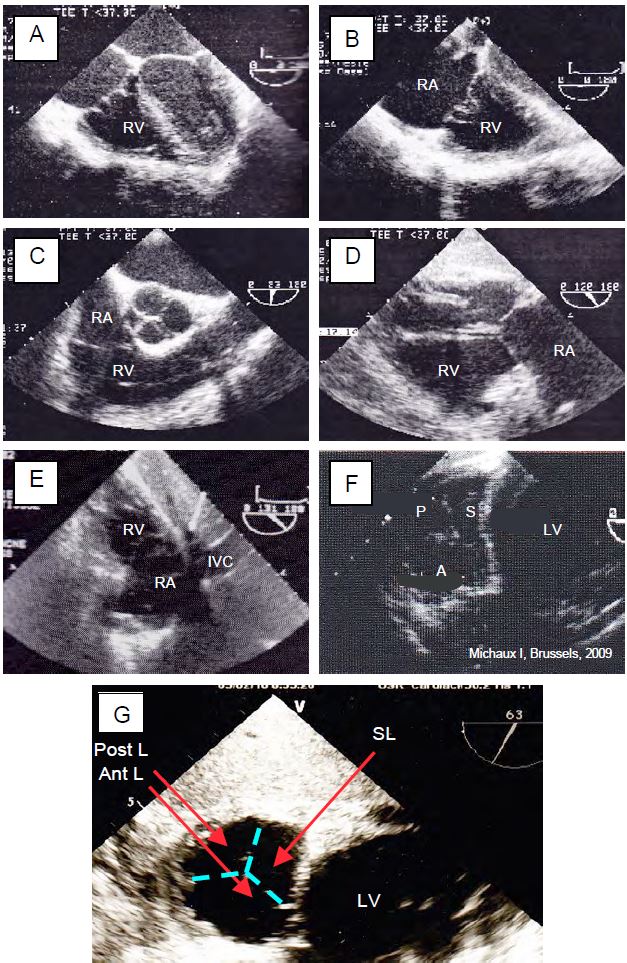
Figure 26.46: Normal TEE images of the tricuspid valve. A: 0° 4-cavity view (septal and non-septal leaflets). B: Deep 0° 4-cavity view (septal and posterior leaflets). C: 60° RV inflow/outflow tract view (posterior and anterior leaflets). D: 120° transgastric VD inlflow/outflow view (posterior and anterior leaflets). E: 130° transgastric view of RV inflow with clockwise rotation of the probe (post and anterior leaflets). F: 30° transgastric short axis view with the 3 leaflets: anterior (A), posterior (P) and septal (S). G: Magnification of the 60° transgastric short-axis view with the 3 leaflets positioned; this image is useful for localisation as the leaflets are thin and often poorly visible.
| Tricuspid valve |
| The valve consists of a large anterior leaflet, a medium-sized posterior leaflet and a smaller septal leaflet. The annulus is ovoid in shape. In 4-cavity view, the normal diameter in diastole is 2.8 ± 0.5 cm (2.5-3.9 cm). Vmax in diastole is approximately 0.5 m/s; maximum gradient is ≤ 2 mmHg. |
© CHASSOT PG, BETTEX D, August 2011, last update November 2019
References
- LANCELLOTTI P, TRIBOUILLOY C, HAGENDORFF A, et al. Recommendations for the echocardiographic assessment of native valve regurgitation: a summary of the EACI. Eur Heart J Cardiovasc Imaging 2013; 14:611-44
- ROGERS JH, BOLLING SF. The tricuspid valve. Current perspective and evolving management of tricuspid regurgitation. Circulation 2009; 119:2718-25
- SHIRAN A, SAGIE A. Tricuspid regurgitation in mitral valve disease. J Am Coll Cardiol 2009; 53:401-8
- ZOGHBI WA, ADAMS D, BONOW RO, et al. Recommendations for noninvasive assessment of native valve regurgitation: a report of the ASE developed in collaboration with the SCMR. J Am Soc Echocardiogr 2017; 30:303-71