The usual surface area of prosthetic valves is 1.5-2.6 cm2 and their mean gradient is 2-6 mmHg. Intraoperative TEE flow measurements may show temporarily high gradients after ECC, either because cardiac output is too high (excessive inotropic effect) or because bypass volume retransfusion is too rapid.
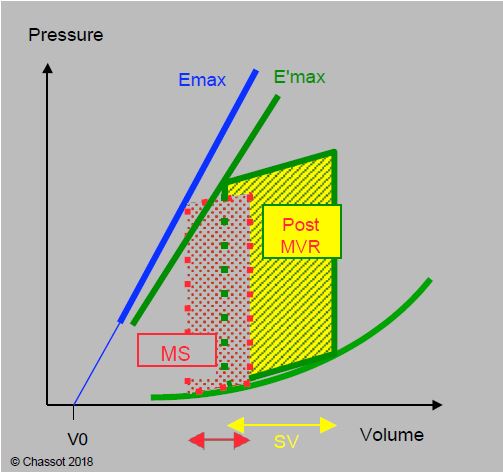
The valve replacement restores the normal diastolic filling of the left ventricle, which is small; this represents a high end-diastolic volume for it. At the end of the bypass procedure, the patient therefore has a congestive type of functional failure (Figure 11.98). Inotropic support is often required. Tachycardia is now beneficial as it reduces Vtd by shortening diastole. If LV function is satisfactory, hypotension is treated with an alpha vasopressor.
Figure 11.98: Pressure-volume loop in mitral stenosis before (MS, in red) and after bypass (green and yellow, after MVR). Stroke volume is increased but shifted towards the flattened part of the compliance curve, i.e. towards high filling pressures; a normal Vtd is equivalent to volume overload in mitral stenosis LV.
Sinus rhythm is beneficial in the first hours and should be maintained as far as possible, even in patients who were in AF preoperatively; these patients usually return to AF within 48 hours postoperatively. Surgical removal of the reentry circuits via an endo-atrial route (Maze procedure) can restore sinus rhythm and, when combined with LA reduction surgery, has a postoperative success rate of 80% [1]. Even if the haemodynamics are improved by a stable atrial rhythm, the restoration of sinus rhythm does not necessarily mean that the atrial contraction is mechanically efficient and contributes significantly to ventricular filling; on echocardiography, there is often no A-flow corresponding to end-diastolic propulsion by the atrium.
Pulmonary resistances and pressures decrease in the first 24-48 hours as the postcapillary component is suppressed; however, PAP does not normalise in the postoperative period as the precapillary component decreases slowly. A non-response in pulmonary haemodynamics indicates fixed and irreversible PHT with a poor prognosis; this can be predicted by the response to an NO• test during preoperative catheterisation. If necessary, active pulmonary vasodilatation should be initiated (see Table 12.6 and Table 12.11).
| Surgery for mitral stenosis: after ECC |
|
Removal of the mitral obstruction results in relative volume overload of the small LV. The postcapillary component of pulmonary hypertension is reduced, but the precapillary component persists postoperatively.
Support:
- Filling restrictions
- Inotropic support (dobutamine), beneficial tachycardia
- Hypotension: alpha vasoconstrictor
- Pulmonary vasodilation and treatment of right-sided failure as required
|
© CHASSOT PG, BETTEX D, August 2011, last update November 2019
References
- NAKAJIMA H, KOBAYASHI J, BANDO K, et al. The effect of cryo-maze procedure on early and intermediate term outcome in mitral valve disease: Case-matched study. Circulation 2002; 106: I-46-52