During the CPB weaning phase, volatile anaesthetic agents are discontinued to avoid the significant myocardial depressant effect that such agents have in young children. Blood products and derivatives must be ready and warmed. The operating theatre is rewarmed. Before stopping CPB, steps must be taken to ensure that: the patient's heart rhythm and rate are restored (bradycardia should be seen as a warning sign), contractility is adequate, temperature is normal (minimum 36°C oesophageal and 35°C rectal), and ventilation is optimal (lung inflation monitored in the operating field, tracheal aspiration). The ventilator is set to induce hypocapnia (PaCO2 30-35 mm Hg) or normocapnia depending on the circumstance; FiO2 is 0.8-1.0. The acid-base balance must be checked to ensure pH ≥ 7.4 to prevent any pulmonary vasoconstriction and enable the catecholamines to take full effect. Young children accumulate significant volumes of interstitial fluid in the pulmonary parenchyma, so modified haemofiltration should be considered for any CPB of a moderate or prolonged duration.
Vasopressors and inotropic agents may be used post-CPB as determined by the observation of the heart in the operating field and on TEE, analysis of central arterial and venous pressure, and haemodynamic variations prompted by the surgery performed. Since they have relatively few β-adrenergic receptors, infants need specific substances that act on the α-adrenergic receptors (epinephrin) or by non-catecholaminergic route (milrinone). Right-side dysfunction is often the dominant factor.
Vasopressors and inotropic agents may be used post-CPB as determined by the observation of the heart in the operating field and on TEE, analysis of central arterial and venous pressure, and haemodynamic variations prompted by the surgery performed. Since they have relatively few β-adrenergic receptors, infants need specific substances that act on the α-adrenergic receptors (epinephrin) or by non-catecholaminergic route (milrinone). Right-side dysfunction is often the dominant factor.
- The contractility of immature hearts is highly dependent on levels of extracellular Ca2+ – CaCl2 0.2 ml/kg to be administered and repeated if necessary (hypocalcaemia, transfusions).
- Milrinone (0.25-0.75 mcg/kg/min) is very useful for young children since it acts by a non-adrenergic route and lowers PVR.
- Epinephrin (0.01-0.5 mcg/kg/min) acts on the β1, β2 and α receptors.
- A milrinone-epinephrin combination is extremely effective for all heart diseases – it is many centres’ preferred inotropic agent for standard or complex cases.
- Dobutamine (5-10 mcg/kg/min) leads to a certain degree of tachycardia and may cause a hypertensive crisis – it is mainly used for simple cases (e.g. isolated VSD).
- In the event of low systemic resistance, norepinephrin (0.05-1.0 mcg/kg/min) may be indicated for maintaining perfusion pressure, and particularly coronary perfusion pressure, if systemic diastolic pressure is too low (0.05 mcg/kg/min), notably in the event of RV dysfunction – ensure that the LV is able to withstand the increased afterload.
- In the event of complete AV block or severe bradycardia, isoprenaline (1 mcg/kg) may be administered pending the installation of a pacemaker – the younger the child, the more his/her blood flow is dependent on his/her heart rate.
- High PAP or subpulmonary ventricular failure are indications for NO• (10-30 ppm).
- Generally, the ventricle most at risk on weaning from CPB is the one that is most hypertrophied or has undergone a ventriculotomy.
Once the pump is withdrawn, the conventional approach to inotropic support in young children is focused on maintaining cardiac output.
- Beta-stimulants administered: dopamine (5-10 mcg/kg/min), dobutamine (5-10 mcg/kg/min), epinephrin (0.1-0.2 mcg/kg/min), isoprenaline in the event of bradycardia (0.01-0.1 mcg/kg/min).
- Milrinone added (0.5-0.75 mcg/kg/min) if beta-stimulation is insufficient – a combination of milrinone + epinephrin is particularly effective.
- Calcaemia (1-1.4 mmol/L), serum magnesium (≥ 0.7 mmol/L) and kaliaemia (4 mmol/L) maintained.
- Main problems of this approach:
- Systolic flow primarily improved, relative reduction in the diastolic flow;
- Tachycardia;
- Increased metabolic demand and mVO2;
- Risk of compromising myocardial perfusion and DO2/VO2 balance.
One innovative approach involves greater focus on diastolic function and organ perfusion pressure [4].
- Limited use of beta stimulants – dobutamine and isoprenaline dropped – epinephrin limited to cardiogenic shock.
- Inodilation: systematic infusion of milrinone (0.75 mcg/kg/min) – initial dose (50 mcg/kg) during CPB. Milrinone may be substituted by levosimendan in high-risk cases.
- Mesenteric and renal vasodilation: low-dose dopamine for its effect on the DA1 receptors (2-3 mcg/kg/min).
- Organ perfusion pressure maintained – vasodilution prompted by the two above-mentioned steps lowers the LV afterload, but may compromise tissue perfusion. It is therefore necessary to add a norepinephrin infusion (0.1-0.4 mcg/kg/min) to maintain perfusion pressure (PP = MAP - CVP) – target values:
- Premature infant: 35 mmHg;
- Full-term neonate: 40 mmHg;
- Child: 50 mmHg;
- Older child, adolescent: 60 mmHg.
- The indication and dosage of norepinephrin are determined by an analysis of the analogical shape of the arterial curve (Figure 12.32C).
- In the experience of the CHUV, this approach has significantly reduced postoperative mortality rates (1.4% versus 7.3%) and duration of ventilation (35 hours versus 69 hours) [4].
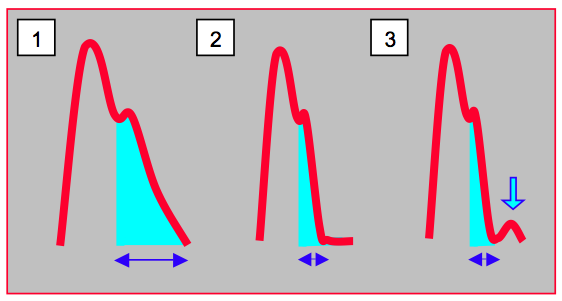
Figure 12.32C: Analogical shape of the arterial curve during diastole. 1: normal curve – the antegrade diastolic flow is proportionate to the area under the diastolic curve (light blue area, blue double arrow). In this case, norepinephrin can be used liberally to improve perfusion pressure if this is too low. 2: the diastolic flow is minimal – the diastolic curve is virtually flat and antegrade flow is non-existent. This shape is typical of hypovolaemia – use of a vasopressor is contraindicated. 3: a norepinephrin infusion initiated in the previous example exacerbates the situation as it prompts a retrograde diastolic flow (arrow) [according to ref 4].
In the hours following CPB, PVR responds to respiratory alkalosis (fall in PaCO2), but is relatively insensitive to oxygen, which is normally a good pulmonary vasodilator [3]. However, patients are ventilated with a high FiO2 (0.8-1.0) to maintain PaO2 of at least 100 mmHg. The persistence of PAH and right-side dysfunction despite the use of pulmonary vasodilators (PGE1, NO•) and inotropic agents (milrinone, epinephrin) may convince the surgeon not to close the pericardium or sternum to avoid a “tamponade effect” on dilated chambers and an increase in intrathoracic pressure, particularly in young children (< 3 kg, < 7 days) [7]. In the event of major stasis, a small relief ASD may be created. The resulting blood flow from the RA to the LA relieves the RV overload and increases LV flow, but at the cost of arterial desaturation [5]. A set of circumstances favours reclosing the sternum 24-48 hours after the operation if the situation has stabilised:
In the hours following CPB, PVR responds to respiratory alkalosis (fall in PaCO2), but is relatively insensitive to oxygen, which is normally a good pulmonary vasodilator [3]. However, patients are ventilated with a high FiO2 (0.8-1.0) to maintain PaO2 of at least 100 mmHg. The persistence of PAH and right-side dysfunction despite the use of pulmonary vasodilators (PGE1, NO•) and inotropic agents (milrinone, epinephrin) may convince the surgeon not to close the pericardium or sternum to avoid a “tamponade effect” on dilated chambers and an increase in intrathoracic pressure, particularly in young children (< 3 kg, < 7 days) [7]. In the event of major stasis, a small relief ASD may be created. The resulting blood flow from the RA to the LA relieves the RV overload and increases LV flow, but at the cost of arterial desaturation [5]. A set of circumstances favours reclosing the sternum 24-48 hours after the operation if the situation has stabilised:
- High risk of ventricular distension;
- High doses of inotropic agents (epinephrin > 0.3 mcg/kg/min);
- Haemodynamic instability, PAH;
- Significantly reduced pulmonary compliance;
- Major tissue oedema;
- Long period of CPB (> 180 minutes), long period of aortic clamping (> 90 minutes);
- Very high LAP, SvO2 < 51%.
An intra-aortic balloon pump cannot be used in young children due to their size, their tachycardia, the flexibility of their aortas, and the presence of any aortopulmonary collaterals. In contrast, ECMO (extra-corporeal membrane oxygenation) is an effective aid in the event of ventricular failure. However, mortality rates remain high when the indication is an inability to wean the patient from CPB. The aim of ECMO is to restore cardiac output, substitute ventilation, reduce inotropic agents, and wait for myocardial functional recovery. Its indications for children are as follows:
- Haemodynamic failure;
- RV failure following severe PAH;
- Long period of aortic clamping;
- Lack of myocardial protection;
- Coronary ischaemia;
- Surgical problems.
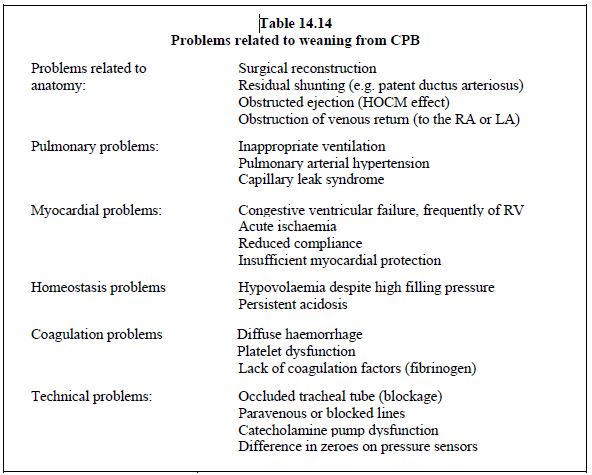
Difficulties weaning children from CPB may also be due to inappropriate or insufficient surgical correction. TEE plays a key role here in determining whether a “second run” CPB is required to improve repair [1,2,6,8]. Non-corrected anomalies have a significant adverse effect on patients’ chances of survival. Potential problems encountered during weaning from CPB are summarised in Table 14.14.
| Weaning from CPB |
|
Ventilation: FiO2 0.8-1.0, ETCO2 30-35 mmHg, NO if PAH or RV failure
Inotropic support: dobutamine, Ca2+, epinephrin-milrinone, levosimendan Vasoconstrictor (norepinephrin) if low SVR or insufficient perfusion pressure (PP = MAP - CVP) Vasodilator if high SVR Pacemaker if heart rate < 100 BPM in young children and < 70 BPM in older children TEE monitoring: ventricular function, blood volume, surgical correction, potential residual defect If refractory ventricular failure: ECMO In neonatal surgery (< 7 days, < 3 kg), do not be afraid to leave the sternum open (24-48 hours) in the event of long periods of CPB, ventricular distension, high doses of inotropes, haemodynamic instability, PAH or reduced pulmonary compliance. |
© BETTEX D, BOEGLI Y, CHASSOT PG, June 2008, last update May 2018
References
- BETTEX DA, PRETRE R, JENNI R, SCHMID ER: Cost effectiveness of routine intraoperative transesophageal echocardiography in pediatric cardiac surgery: a ten-year experience. Anesth Analg 2005; 100:1271-5
- BETTEX DA, SCHMIDLIN D, BERNATH MA, PRETRE R, HURNI M, CHASSOT PG. Intraoperative trasnesophageal echocardiography in pediatric congenital heart surgery: A two-center observational study. Anesth Analg 2003; 97:1275-82995; 60:S539-42
- GIGLIA TM, WESSEL DL. Effects of oxygen on pulmonary and systemic hemodynamics in infants after cardiopulmonary bypass. Circulation 1990; 82(suppl III):III-78
- HOSSEINPOUR AR, VAN STEENBERGHE M, BERNATH MA, et al. Improvement in perioperative care in pediatric cardiac surgery by shifting the primary focus of treatment from cardiac output to perfusion pressure: are beta stimulants still needed ? Cong Heart Dis 2017; 12:570-7
- LAKS H, PEARL JM, HAAS GS, et al. Partial Fontan : Advantages of an adjustable interatrial communication. Ann Thorac Surg 1991 ; 52 :1084-95
- RANDOLPH GR, HAGLER DJ, CONNOLLY HM, et al. Intraoperative transesophageal echocardiography during surgery for congenital heart defects. J Thorac Cardiovasc Surg 2002; 124:1176-82
- SAMIR K, RIBERI A, GHEZ O, et al. Delayed sternal closure : a life-saving measure in neonatal open heart surgery : could it be predictable ? Eur J Cardiothorac Surg 2002 ; 21 :787-93
- UNGERLEIDER RM, KISSLO JA, GREELEY WJ, et al. Intraoperative echocardiography during congenital heart operations: Experience from 1000 cases. Ann Thorac Surg 1995; 60:S539-42